Pleural effusion, popularly known as water in the pleura or water in the lung, is the name given to the abnormal accumulation of fluid in the pleura, a thin membrane surrounding the lung.
Pleural effusion is not a disease, but a common manifestation of several different diseases. Therefore, once diagnosed the presence of stroke, the next step is to investigate its cause.
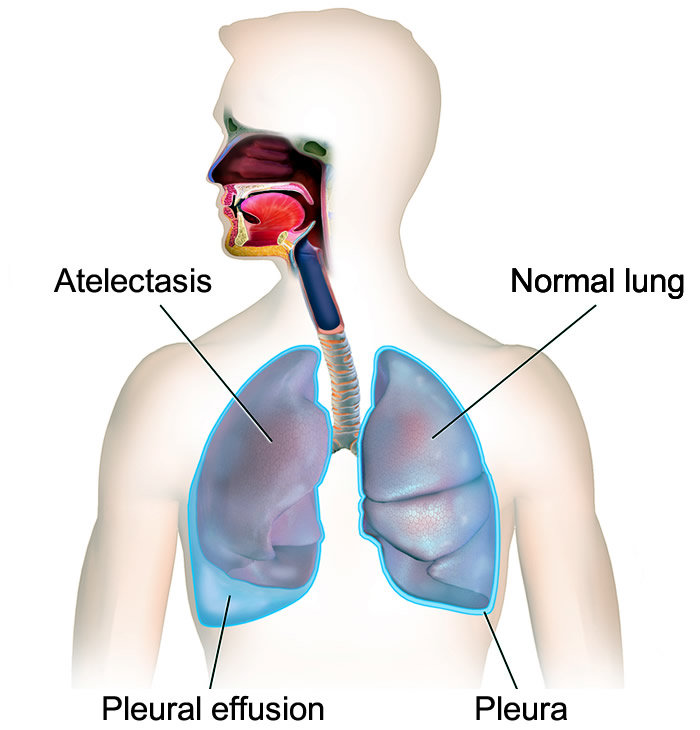
Just as the meningeal is the membrane that surrounds the brain and the pericardium is the membrane that surrounds the heart, the pleura is the name given to the membrane surrounding the lungs.
Note: The pleura of the lung is a pleonasm since there is no pleura other than the one involving the lung. The correct term is simply pleura.
The pleura is composed of two layers, the visceral pleura that is the inner layer and is glued to the lung, and the parietal pleura, the outermost layer that is in contact with the anatomical structures around the lungs.
Between the two layers of pleura there is a minimum space of 20 micrometers (0.02 mm), called the pleural cavity, or pleural space. Inside it is a tiny blade of liquid, which plays the role of lubricant, preventing the friction between the two layers of the pleura when the lungs fill and when they are exhausted of air. This fluid receives the obvious name of pleural fluid.
The normal volume of fluid within the pleural cavity is approximately 0.2 ml per kg of body weight, ie about 12 ml in a 60 kg individual.
The pleura is highly vascularized and its fluid is constantly renewed at a rate of 0.6 ml/hr. The blood and lymph microvessels that irrigate the pleura are responsible for bringing and carrying the pleural fluid, always maintaining a constant volume within the cavity. When there is a disturbance of this balance, there is fluid retention in the pleural space and the effusion is formed.
Pleural effusion is basically divided into two types, this distinction being important for establishing the cause.
1) Transudate - The transudative pleural fluid is clear and transparent, without cells, with a low concentration of proteins, indicating an accumulation of a liquid similar to normal pleural fluid.
Pleural effusion that manifests with transudate-like fluid is usually caused by:
In general, any disease that develops with ascites can also occur with pleural effusion, since there is communication between the abdominal cavity and the thorax.
2) Exudate - Exudative pleural fluid is rich in proteins and inflammatory cells, has a more viscous and opaque appearance, sometimes with signs of mixed blood, and in cases of infections it may present as a collection of pus.
Pleural effusion that manifests with an exudate-like fluid usually occurs by inflammation of the pleura and may be caused by several different groups of diseases, including infections, systemic diseases, and cancers. The most common diseases that cause exudative pleural effusion are:
Intra-abdominal complications such as peritonitis or abscess
Ovarian hyperstimulation syndrome
Radiotherapy
The distinction between exudate and transudate is made through the dosing of proteins in the liquid, explained further below.
When the accumulation of a purulent fluid occurs, we call it pleural empyema. There are also other types of fluid that can accumulate in the pleura, such as:
Blood, called hemothorax, which usually occurs in the penetrating traumas of the lung.
Urine, called a urinothorax, a rare condition that can occur in urinary tract obstructions.
Triglycerides and lipids, called chylothorax, usually caused by obstruction of the lymphatic vessels of the pleura.
The greater the stroke, and the faster it forms, the more symptoms it will cause.
When looking at the illustration to the side demonstrating the compression of a lung by excess pleural fluid, it is not difficult to understand why the most common symptom of pleural effusion is shortness of breath, called dyspnea.
When the stroke suddenly appears, the shortness of breath is more evident. When it forms slowly, and if associated with other diseases that also cause shortness of breath like heart failure, it may go unnoticed for some time.
Some pleural effusions can be as bulky as 4 liters, which is enough to completely compress the affected lung.
Another common symptom of pleural effusion is the chest pain that usually occurs when the pleura is irritated. This is a stabbing pain that worsens every time the patient breathes deeply. This type of pain is called pleuritic pain. Often there is also an irritative dry cough.
The pain and shortness of breath are basically the two symptoms of the stroke itself. The other symptoms that usually accompany the condition usually occur due to underlying disease, such as fever and cough in pneumonia, cough with blood streaks in lung cancer, ascites in cirrhosis, swollen legs in heart failure, and so on.
A well-done physical examination, with good lung auscultation, is capable of suggesting the presence of pleural effusion whenever there is more than 300 ml of accumulated fluid. Excess fluid is lodged in the lungs and back, and the lung sounds are inaudible.
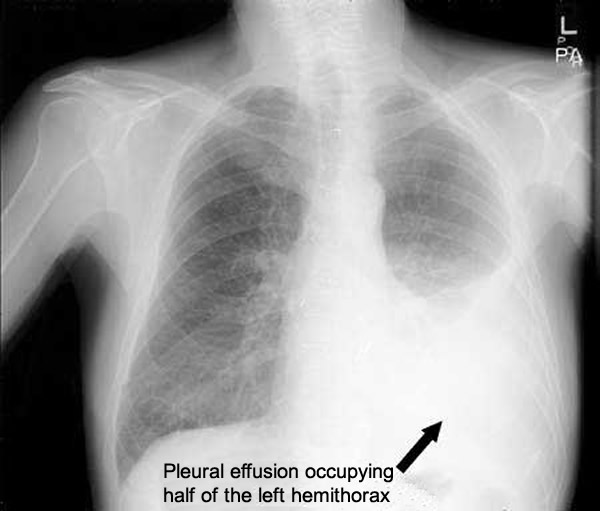
When clinical history and physical examination suggest the presence of pleural effusion, confirmation can be made with a simple chest X-ray. The pleural effusion appears as a large white spot where only the air-filled lung should be seen.
To be detected by plain radiography, the pleural effusion should have at least 75 ml of fluid. When in doubt, one option is to make another x-ray with the patient lying on its side, causing the fluid to flow along the ribs. This technique allows to diagnose spills less than 50 ml.
Exams such as computed tomography and ultrasound can detect collections of minimal fluids, such as a mere 10 ml.
Once the pleural effusion is diagnosed, unless its cause is obvious, such as in cirrhotics with large ascites, decompensated nephrotic syndrome or severe heart failure, its liquid must be analyzed in order to determine its composition.
The only way to approach pleural fluid is through a procedure called thoracentesis, which involves inoculating a needle between the patient's ribs until the pleural space is reached. Usually between 50 and 100 ml of the effusion is collected.
The collected liquid can be analyzed in order to determine the presence of exudate or transudate, cancer cells and bacteria.
In addition to thoracentesis for diagnosis, in cases of massive pleural effusion, a small tube can be implanted to drain larger volumes of fluid in order to clear the affected lung.
The main complications of thoracentesis are bruising at the puncture site, contamination of pleural effusions from skin bacteria, and pneumothorax.
If the above exams do not identify the cause of the pleural effusion, a thoracoscopy can still be performed, with the introduction of an endoscope into the pleural cavity for visualization of the pleura and lungs and eventual biopsy.
As it was said at the beginning of this text, the pleural effusion is not a disease in itself, but a sign of a disease. Therefore, simple drainage of the fluid is only a palliative procedure, since if the cause is not treated, the major hypothesis is that the stroke will form again.
The pleural effusion will be resolved as soon as the disease causing it is controlled. Infections are controlled with antibiotics, renal failure with hemodialysis, autoimmune diseases with immunosuppressants, etc.
In some situations, when the underlying disease has no effective treatment, as in many cases of metastatic cancers, one option to avoid the repeated formation of pleural effusions is pleural cavity sclerosis. An irritating substance is injected into the pleura causing a great cicatrization of the same and adherence of the parietal and visceral leaflets, thus eliminated, the pleural space.