The inflammatory process leads to the formation of edema, increased mucus production and spasm of the respiratory tree, hindered passage of air through the lungs. This process is called bronchospasm and is characterized by difficulty in breathing, wheezing, coughing and feeling of heaviness in the chest.
In this article we will explain asthma by addressing its causes, symptoms, diagnosis and treatment options.
In order to explain what is asthma and how it arises, we must first go through some basic aspects of the anatomy of the respiratory tract.
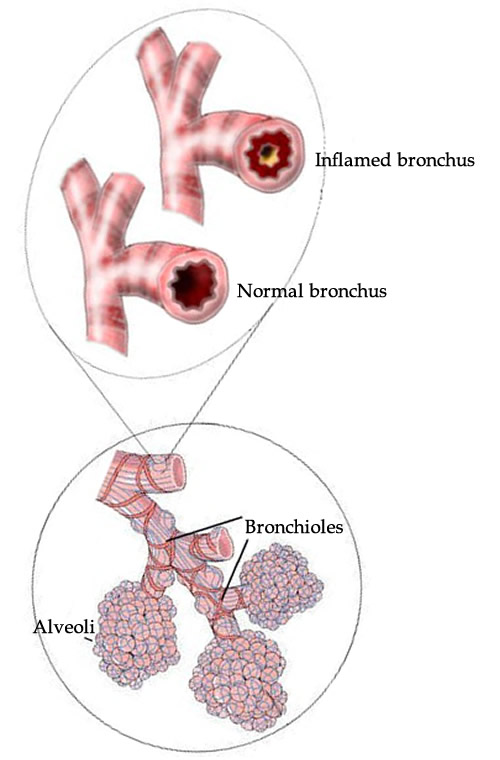
When we breathe, air enters through the nose (or mouth), passes through the larynx and trachea reaches a caliber tube that leads to the lower respiratory tract. The trachea bifurcates, forming the main bronchi, each heading towards one of the lungs. As will advance to the lungs, the bronchi will branching into increasingly smaller segments called bronchioles, in turn, terminate in the alveoli occurs structure where oxygenation of the blood. The terminal bronchioles air channels are so small, having a diameter of only 0.5 millimeters.
For reasons not yet clear, patients with asthma develop chronic inflammation in their small airways. This inflammation causes the asthmatic is a person with an extremely sensitive lung. simple environmental stimuli, such as exposure to pollen, smoke, dust, cold, etc., which are easily tolerated by the lungs of healthy people, often cause severe allergic reaction in the lungs of patients with asthma. This overreaction leads to edema formation in the bronchioles, excessive mucus production and spasms of the muscles of the bronchi (bronchospasm), factors which cause a large reduction in airway caliber, obstructing the passage of air.
The individual with asthma crisis has trouble inspiring, but even more difficult to expire, causing part of the inhaled air entrapment within the alveoli, causing hyperinflation of the lungs.
Fortunately, this obstruction caused by the reduction in airway caliber is a reversible process, an essential feature that distinguishes asthma from chronic bronchitis and emphysema, diseases known as COPD (chronic obstructive pulmonary disease).
Asthma is a disease that can fade or show great improvement in adolescence. In some cases, it disappears and returns years later adult life; in others, it goes away and never comes back. There are also patients who will develop asthma for the first time only in adulthood, some only in the 3rd age.
Asthma is a disease that can occur at any age but is most common in children. In 75% of cases, it manifests itself before the age of 7. It is estimated that the disease affects about 10% of the pediatric population and 5% of adults.
The most common signs and symptoms of asthma are breathlessness, bronchospasm (characterized by wheezing during breathing) and cough. Many patients also complain of heaviness or pressure in the chest. A typical feature of asthma is worsening of symptoms at night.
Asthma usually manifest in attacks that come and go, and are triggered by some known factors such as respiratory viruses, smoke, cold, dust, by animals, etc. When out of the crisis, the patient usually has no symptoms, but some degree of bronchospasm usually present, especially in patients with more severe asthma. In general, these individuals adapt to this slight decrease in the caliber of their airways and not refer complaints during their day to day, unless you need to make some effort.
Asthma is usually classified as intermittent, mild persistent, moderate persistent or severe persistent. Clinically, each class typically have the following characteristics:
1. Asthma intermittent
Asthma attacks appear with a frequency less than 2 days per week, the patient wakes up less than 2 nights per month crises, the inhaler bronchodilator is only necessary in less than two days a week and asthma often not influence the activities everyday.
2. Mild persistent asthma
Asthma attacks appear with a higher frequency than 2 days a week (but not every day), the patient wakes up at least 3 to 4 nights per month crises, the inhaler bronchodilator is required more than 2 days a week ( but not every day and not more than 1 time per day) and asthma can cause mild limitations in activities of daily life.
3. Moderate persistent asthma
Asthma attacks appear daily, the patient wakes up more than 1 time per week with crises, puffer bronchodilator is required every day and asthma can cause limitations in activities of daily life.
4. Severe persistent asthma
Asthma attacks appear daily, more than once a day, the patient wakes up every night with crises, the inhaler bronchodilator is required several times a day and asthma may cause severe limitations in daily activities.
The breath test, which will be explained later, are also used to assist in the degree of severity of asthma.
Signs of severity of an asthma attack
Some patients in addition to having moderate to severe persistent asthma, may also have severe acute asthma attacks requiring prompt medical attention. The signals of gravity of an asthma attack include:
Greater effort to breathe.
Purplish or bluish lips.
Anxiety Crisis.
Difficulty speaking.
Intense sweating.
Sharp use of chest muscles, abdominal or neck during breathing.
We do not know exactly what leads an individual to developing asthma. We know, however, that there is a strong genetic factor because the disease typically affects several members of the same family. If one parent has asthma, the child's risk of having the disease is 25%. If the father and mother are asthmatics, the risk rises to about 50%.
The relationship with allergic processes is also very clear and very common the association between asthma and other allergies, such as atopic dermatitis, allergic rhinitis, urticaria, etc.
obese patients, smokers, passive smokers, people whose mother smoked during pregnancy, babies with low birth weight, people exposed to smoke from fire, patients with gastroesophageal reflux, workers exposed to certain chemicals or contact with pesticides also increase the risk of an individual developing asthma.
Triggers of asthma attacks
In general, in patients with asthma, asthma attacks are triggered by known factors, which should be avoided whenever possible. In the vast majority of cases, the predisposing factors are substances sucked the air. Among the most common triggers of asthma attacks include:
Some people develop asthma attacks after practicing physical activities. The exercise-induced asthma name is not the most appropriate, as it may lead to the false understanding that exercise may cause asthma. In fact, the physical activity can trigger asthma attacks in a patient previously asthma. So the more accurate term is exercise-induced bronchospasm.
In most cases, the physical effort practice exacerbates an existing and symptomatic asthma. However, there are cases where the patient has asthma attacks only after physical activity. The effort is the only trigger trigger bronchospasm.
The bronchospasm usually appear 10 to 15 minutes after the onset of moderate to intense activity. In general, the symptoms disappear after 30 minutes of rest. physical activities in cold environments increase the risk of exercise-induced asthma.
The use of bronchodilators 10 minutes before the physical activity helps to prevent bronchospasm and prevent the patient becomes inactive.
The investigation of a patient with suspected asthma is predominantly focused on the assessment of symptoms and tests that evaluate lung function. Other examinations, including chest X-rays, blood tests and allergy tests are useful in selected patients, but they can not by itself establish or refute the diagnosis of asthma.
In children, especially the young, asthma can be difficult to diagnose because many other respiratory diseases can cause similar symptoms and the tests that are described below are not usually suitable for children.
In small, so the pediatrician can choose to indicate a therapeutic trial if suspected of asthma. If symptoms improve with treatment for asthma, the more likely that the child actually has asthma.
Spirometry
Spirometry is a test done to evaluate how well your lungs work. The test is very simple. To do so, you need well fill his lungs with air and then blow as soon as possible in mouth which is connected to a computer. The spirometer evaluates two measures:
the volume of air you can exhale in the first second of exhalation, called forced expiratory volume in one second or FEV1;
the total amount of air you can exhale, called forced vital capacity or FVC.
To obtain a more reliable reading, the doctor may ask you to blow in spirometer more than once. Once the physician to assess the examination was carried out satisfactorily, it will compare the results with the reference values, which are the average values for people of the same age, sex and height. Thus it is possible to assess for signs of airway obstruction.
Then, the doctor will repeat the test after administration through an inhaler (the famous puffer for asthma) a bronchodilator, used to dilate the airways of the lungs. Patients with asthma often have a significant improvement in spirometry results after bronchodilator use, a result that is not observed, for example, in patients with chronic bronchitis (COPD).
Peak flow
The peak expiratory flow meter, also called meter peak flow , is an alternative and simpler way to assess airway obstruction. The result obtained by measuring peak flow is called peak expiratory flow (PEF).
While spirometry the patient must blow into a mouthpiece that is connected to a computer, the meter peak flow is a small handheld device, you might have at home, and is used to measure how fast you can blow air your lungs in one breath, short and explosively. As in spirometry, the results should be compared to reference values. An improvement of at least 20% in profit after bronchodilators speaks strongly in favor of asthma.
This test, although simple, requires a little practice to be done correctly and does not provide results as reliable as spirometry. So it ends up being more useful in the monitoring of patients who already have established the diagnosis of asthma. As can be done at home at any time, it is useful to assess lung function throughout the day. Knowing the usual pattern of EFP helps the patient to recognize when your asthma is getting worse.
If the patient suspects that there is a trigger factor of asthma in their work, it may take the meter peak flow with you to work and compare the results before then.
Treatment of asthma is a complex subject and deserves a unique article. What we do next is a summary of the most widely used options.
1. Bronchodilators beta2-agonists
Bronchodilators, beta-2 agonists are drugs that act by relaxing the bronchial muscles, increasing their size and facilitating the passage of air. Like asthma obstruction mechanism is bronchospasm, bronchodilators are great options to reverse the symptoms of the disease. Beta2-agonists, though they are effective in fighting the symptoms and have rapid onset of action, do not act directly on the causes of asthma, which is inflammation of the airways.
Bronchodilators are administered by inhalation. There are short-acting bronchodilators (4 to 6 hours) such as salbutamol, fenoterol, and long-acting bronchodilators (12 to 24 hours), such as salmeterol and formoterol.
2. Corticosteroids Inhaled
Corticosteroids are drugs derived hormone and Cortisol have potent anti-inflammatory effect. For this reason, inhalation corticosteroids are often used in the treatment of asthma.
Among the corticoids options Inhaled most used include: fluticasone, budesonide, beclomethasone, flunisolide, ciclesonide, triamcinolone acetonide and mometasone.
Unlike corticosteroids taken orally or intravenously, inhaled corticosteroids have a relatively low risk of side effects and are generally safe for everyday use and long term.
Inhaled corticosteroids are often used in combination with beta-2 agonist long term.
3. Modifiers leukotrienes
Leukotriene modifiers are drugs used orally in tablet or syrup, which help to open the airway, decrease inflammation and decrease mucus production. They are less effective than corticosteroids, therefore, not usually used alone in treating asthma, but rather as a supplementary drug.
Among the options available in the market may include: montelukast, zafirlukast and zileutona.
4. Theophylline
Theophylline is a drug oral bronchodilator effect. Widely used in the past, she is currently a complementary treatment option.
5. Omalizumab
Omalizumab is a relatively new drug indicated for the treatment of allergic asthma that can not be controlled with corticosteroids. The drug is usually administered subcutaneously every 2 or 4 weeks.