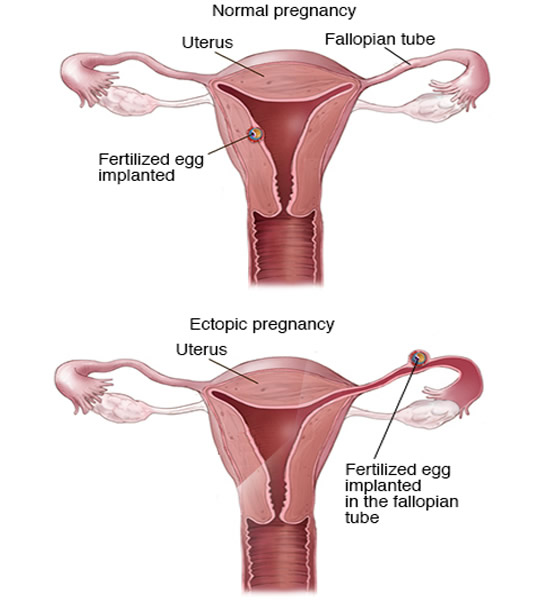
Ectopic pregnancy is a problem that arises when the fertilized egg implants itself wrongly in other structures than the uterus. The most common form of ectopic pregnancy is tubal pregnancy, which occurs within the fallopian tubes.
The normal process of forming a pregnancy comprising the steps of:
Ovulation → migration of the egg to one of the fallopian tubes (fallopian tubes) → ovum encounter with a sperm → fertilization of the ovum → migration egg (fertilized egg) from the fallopian tube toward the uterus → implantation of the egg in the uterine wall.
Ectopic pregnancy occurs when something wrong happens in the last 2 steps. In 98% of cases of ectopic pregnancy, the egg does not travel all the way and end up staying early in the wall of the tubes. In the remaining 2%, egg implantation occurs other structures such as ovarian, cervical or abdominal cavity.
Ectopic pregnancy is a pregnancy without a future. The egg plus can not develop normally outside the uterus, can also cause serious damage to structures surrounding it. If left untreated, ectopic pregnancy carries a high risk of death. Until the early twentieth century, mortality was above 50%. Fortunately, with the current techniques of diagnosis and treatment, the mortality rate of ectopic pregnancy has dropped to less than 0.05%.
Pregnancies outside the uterus correspond to about 1 to 2% of all pregnancies. The diagnosis is usually made around the eight weeks of pregnancy.
Several risk factors have been identified, some of them more important than others. In most cases, the problem lies in the tubes, which are inflamed, infected or structurally damaged, make the egg is difficult to complete their migration towards the uterus.
Let's quote some of the known risk factors. In general, all of them, directly or indirectly, are related to infection or anatomical problems of the tubes.
1) Factors that greatly increase the risk of ectopic pregnancy:
Inflammation or active infection of the fallopian tube (salpingitis).
Structural lesion of fallopian tube by previous inflammation.
Previous surgery of the tubes.
The tube ligature faults.
Pregnancy Episode previous ectopic.
Use of IUD (IUD rarely fails, but when this occurs, the risk of ectopic pregnancy is very high).
2) Factors moderately increase the risk of ectopic pregnancy:
In some women, the early symptoms of ectopic pregnancy are not different from those that occur in a topical pregnancy, such as missed periods, nausea, breast enlargement, to pee all the time, etc. Just as in normal pregnancies, the pregnancy test is also positive pregnancy outside the womb.
In most cases, however, women have no signs or symptoms initially and did not even suspect that they are pregnant when the first signs of ectopic pregnancy occur around the 6th to 8th week of pregnancy. It is very common to patients with ectopic pregnancy seek medical attention with the following triad of symptoms:
Not always these three symptoms are present at the same time, but they are the most common of an ectopic pregnancy.
Abdominal pain is usually unilateral, but it can be diffused, but with greater intensity on the side of the affected tube. The pain varies from moderate to high intensity, depending on the degree of disease progression. If there is bleeding the tube, the patient may complain of pain radiating to the shoulder or have intense desire and pain when defecating. Physical examination can feel a mass in the inguinal region (groin).
If there is rupture of the tube (ruptured ectopic pregnancy), abdominal pain becomes intense, and appear signs of peritonitis (inflammation of the peritoneum, the membrane that covers the intra-abdominal organs). In these cases, bleeding can be bulky and patient at risk of entering circulatory shock.
The vaginal bleeding, ectopic pregnancy usually mild, but in some cases it may be intense. Its color can be bright red or very dark. Bleeding is usually different from menstrual bleeding.
It is very difficult to establish the diagnosis of ectopic pregnancy only the symptoms. Generally, the diagnosis is obtained after a gynecological examination and transvaginal ultrasonography. A positive hCG Beta, which shows elevated values slower than usual, and the absence of embryo inside the uterus are important tips in the framework of research. When pregnancy is very early, it is not always easy to identify the location of the ectopic embryo. Sometimes you have to wait a few days to be able to define the diagnosis with certainty.
No ectopic pregnancy has a future, and the risk of mother's death, if left untreated, is very high. Therefore, all treatment modalities aimed at the removal of the embryo before major complications arise.
There is surgical and medical treatment for ectopic pregnancy.
1. Drug treatment for ectopic pregnancy
If ectopic pregnancy is diagnosed early, it is possible to administer drugs which prevent development of the embryo, causing the same involua. The commonly used drug is methotrexate intramuscularly in a single dose. Currently, about one third of ectopic pregnancies are treated with methotrexate.
The indications for drug treatment are: an embryo less than 4 cm, absence of heartbeat of the fetus, no rupture signs of horn and beta hCG with value less than 5000 mIU / mL.
After injection, the obstetrician accompanying the pregnant woman with serial measurements of beta hCG. The goal is that the values begin to fall and reach zero. If after the first injection there is no response, a second dose of methotrexate can be administered.
2. Surgical treatment for ectopic pregnancy
Historically the treatment of ectopic pregnancy was always done with surgery to remove the evil implanted embryo. Currently, surgery is the treatment of choice for nearly 60% of cases.
In most situations, the surgery is done laparoscopically. The goal is to remove the embryo and repair the damaged area of the tube.
In emergency cases, with massive bleeding or rupture of the tube, the traditional open surgery is the most appropriate way. It is not always possible to repair the tube, and it may have to be removed to control. Even with the removal of the tube, the woman can get pregnant later if the tube on the other side is healthy.