Learn all about the headache, the famous headache. What are the most common causes and when you should start worrying?
A headache is the most common medical complaint. It is difficult to find someone who has never had one in life.
The headache is a symptom that often causes concern among patients. It is not uncommon to get people terrified of the possibility of a serious disease such as aneurysm or tumor, when the doctor requests a CT scan anyway, when in fact it is just a simple headache, easily diagnosed clinically.
Although it's very common that people know very little about the headaches and think that all are equal. In fact, there are several causes for headache. The vast majority are benign and 90% are caused by one of these three syndromes.
Still there are the headaches related to sinusitis and back problems.
Contrary to what one might imagine, vision problems as nearsightedness, farsightedness and astigmatism are not common causes of headache. There is also a myth that chronic headache and liver problems are connected.
Contrary to what many people think, migraine is not the term for headache of great intensity. Migraine is a specific type of headache.
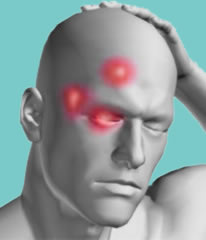
It is characterized by being unilateral (70% of cases), throbbing, at first gradual, often achieving great intensity, worsening in bright light and noise, can be accompanied by nausea, vomiting or dizziness. The pain usually worsens with head movement and physical exertion. Also the hypersensitivity of the scalp is common, causing pain with a simple brushing of hair. Seizures can last from 4 hours to 72 hours.
Migraine is 3 times more common in women, occurs mainly between 20 and 40 years and is often hereditary. Obese people have a higher incidence. The attacks may be so frequent as to appear more than 4 times per month.
20% of patients have a symptom that is characteristic of migraine, called aura. It is neurological signs that precede the onset of pain. They are typically bright or luminous rays in sight and tingling in any part of the body that occur before the onset of headache. Sometimes the aura may appear as muscle weakness, partial loss of vision and changes in speech that are very frightening for patients as it can anticipate a stroke. The difference is that the auras last for an average of only 20 minutes and usually disappear spontaneously after the onset of pain. Eventually some symptoms of weakness may take longer to disappear.
There are several subtypes of migraine, more rare, which can cause neurological symptoms that do not fit the definition of aura. These signs and symptoms are very similar to those of a stroke. Often only a neurologist can tell them apart.
MRI
The cyclic vomiting syndrome is a rare condition that usually occurs in people with migraine and is characterized by repeated episodes (3-4 times per year), bouts of vomiting that can last 3-6 days. Sometimes you need to hospitalize patients for control of the holding and hydration and correction of electrolyte disturbances.
Migraine headaches can be triggered by stress, menstruation, hunger, exercises, contraception, perfume, smoke, soft drinks or foods that contain nitrites, aspartates, glutamate or tyramine.
The diagnosis is clinical. Examinations with MRI and CT scans are performed only when the condition is unusual and there is suspicion of another diagnosis.
There is no cure for migraine, but the treatments available today are very effective.
A tension headache is the type of headache most common in the population. It affects more women than men. The classification subdivides the latest in 3:
Infrequent tension headache - less than 1 episode per month
Frequent tension headaches - from 1 to 14 episodes per month
Chronic tension headache - more than 15 episodes per month
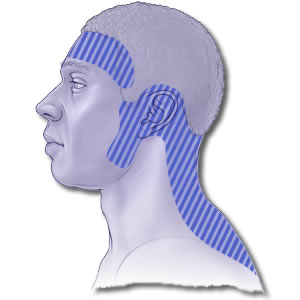
The typical presentation is a moderate headache, non-pulsatile, with no other associated findings, unlike migraine. It may last from 30 minutes to 1 week. The most common complaint is pain in a tightening across the head. It is also very common to find the muscles of the head, neck and shoulders tense and contracted.
Other symptoms include insomnia, fatigue, irritability, poor appetite, difficulty concentrating. Stress is the main trigger of the crisis.
Treatment is analgesics or anti-inflammatory pills.
As a headache can be very frequent, there is a group of patients who end up abusing the pain medication. This behavior can lead to drug-induced headache. Patients have headaches despite the use of analgesics, suggesting a framework of tolerance. There is a debate whether the painkillers themselves can cause headaches. To avoid this complication, those with frequent headache attacks (regardless of type) must consult a neurologist.
A cluster headache is less frequent and more severe of the three main types of primary headaches. It occurs in cycles of crises that can last several weeks by bouts that can last months to years. It is more common in men. An attack may last from 30 minutes to 3 hours and place up to 3 times per day.
The pain is typically unilateral and unlike that of migraine may vary in style, headaches often attack in the same direction. It is a sudden onset of pain, which quickly reaches its greatest intensity, often excruciating, located around one eye.
It is usually associated with tearing and redness of the affected eye. Stuffy and/or runny nose can also be present.
There is a clear association of precipitating factors as in migraine and tension. Alcohol consumption and cigarette triggers a crisis.
Interestingly it is a headache that responds to oxygen administration, in addition to common analgesics.
As explained before, the vast majority of the episodes of headache are caused by benign pathologies. But even people with a history of chronic headaches are frightened by some crisis. The fear of all is that an unidentified illness, such as a tumor or aneurysm, can be the cause of the headache.
It is impracticable to conduct computed tomography (CT) in all people with headache. In general, a good clinical history and physical examination are sufficient to define whether there is need to perform an imaging study.
It is important to bear in mind the main characteristics of primary headaches described above, not to confuse them with the serious causes. The main warning signs are:
Sudden Onset: persistent headaches of sudden onset, reaching its greatest intensity in a few seconds may indicate rupture of aneurysms or venous thrombosis. It is important to remember that cluster headache may have these characteristics, however, it usually lasts a few hours, has typical location and signs such as watery eyes and red eyes. Migraine typically begins as a mild to moderate pain and worsens with the course of hours.
Worst headache of life: When the patient reports that the current framework is by far the worst headache of their life, or a headache completely different from the usual one, should have more attention. Bleeding and infection may be the cause. These complaints in cancer patients, AIDS and immunocompromised are particularly worrying.
Concomitant infections: Patients who present a profile of sinusitis, otitis, skin infections on the face have a higher risk of developing brain abscesses and meningitis. Infections after implantation of piercings can be the gateway.
Fever: The presence of severe headache associated with fever without apparent cause, especially if there is neck stiffness, indicates meningitis. It is important to remember that fever alone can cause headache. Do not confuse the flu with something more serious.
Medications: Some patients use medications such as corticosteroids, which facilitate infections, and anticoagulants to facilitate bleeding.
Changing the state of consciousness: Obviously, patients who fall into a coma, have seizures, sudden confusion or neurological deficits should seek immediate emergency service.
Trauma: Headaches that occur after trauma should be evaluated more carefully, especially in the elderly people due to the risk of intracranial hemorrhage. Some people develop chronic headaches after a trauma to the skull.
Family history: Patients with first-degree relatives who suffered ruptured aneurysms should also be tested more carefully.
Special attention should also be drawn to other signs, like a headache that awakens the patient, headache which characteristics do not fit in any of the primary causes, worsening of pain on exertion (remember that migraine may have this feature), onset of headache after 50 years or visual changes that may suggest glaucoma.
There is no defined protocol for when to ask for a CT scan. Some tables are obvious, as in neurological disorders in others - more questionable. It depends on the good judgment of the physician and the patient's condition.
My sister-in-law and my husband's aunt suffer from migraine. Besides, the examination with MRI proved that she had aneurysm. Thanks God, none of my children have these problems, but my granddaughter showed some symptoms of migraine. Are my sister-in-law and her aunt considered to be her first-degree relatives?
replyquote
Sophie
13 May 2012
My sister said, that the only remedy to get rid of migrain is to cause a gag reflex. She said she used to feel much better after vomitting.