Renal Osteodystrophy - Bone Disease in Renal Failure
In this text we will address dietary care, existing treatments and the consequences for the body of poor control of calcium and phosphorus metabolism in patients with advanced renal failure.
Phosphorus is a mineral salt vital to the basic functions of the body. Its main role, along with calcium, is in the formation and maintenance of bones and teeth. 85% of our phosphorus is stored in the bones. This mineral is also important in the function of the muscles, in the control of blood pH, in the generation of energy, in the production of hormones, etc.
When we talk about controlling the metabolism of phosphorus, we have to think about controlling the metabolism of bones. This relationship is complex and involves several mechanisms, among them:
Parathyroid hormone (PTH) (hormone produced in the parathyroid glands)
Blood calcium concentration
Renal function
Blood phosphorus concentration
Understanding some concepts may help to understand why some treatments and dietary restrictions of patients with renal failure. Before we talk specifically about phosphorus control, we will describe some important points of bone health.
The problem is that both pathways produce only the inactive form of vitamin D. In order for it to perform its functions in the body, activation by the kidneys is necessary. So ultimately, the important vitamin D is active vitamin D, produced by the kidneys.
Patients with chronic renal failure have diseased kidneys that, among other failures, are not able to produce sufficient active vitamin D.
The main function of vitamin D is to maintain normal calcium and phosphorus concentrations in the bone, keeping it healthy and strong. Vitamin D also inhibits the production of PTH, a hormone that contributes to bone demineralization.
There are already medicines that contain active vitamin D and can be used to control bone disease in renal failure. The most common drugs are calcitriol, paricalcitol, alfacalcidol and doxecalciferol.
The main adverse effect of vitamin D treatment is increased blood levels of phosphorus. Therefore, in order to use this class of drugs, it is necessary to have the phosphorus well controlled (I explain as at the end).
The parathyroid glands are 4 small glands located on the thyroid.
Note: Thyroid and parathyroid are organs with completely different functions, although they are anatomically glued and have similar names.
Parathyroid hormones produce a hormone called PTH, which is responsible for controlling blood levels of calcium, phosphorus, and vitamin D. PTH acts by removing calcium from bones, increasing renal phosphorus clearance, and stimulating renal production of activated vitamin D.
Lack of vitamin D and excess phosphorus in the blood that occur in renal failure stimulate PTH production. The problem is that with diseased kidneys, however PTH there is, there is no way to produce vitamin D or excrete phosphorus in the urine. The only action that PTH can exert is to remove calcium from the bone. We then enter into a vicious cycle. As phosphorus does not go down and vitamin levels do not rise, parathyroid hormones are being stimulated indefinitely, leading to a picture we call hyperparathyroidism.
Currently there is a drug called cinacalcet (Mimpara) that acts directly on the parathyroid, inhibiting the secretion of PTH.
So far we already know 2 things about the patient with kidney failure:
Does not produce enough vitamin D to keep your bones healthy
It produces an excess of PTH that leads to the demineralization of the bones
When the kidney starts to get sick, phosphorus excretion in the urine begins to fail. At this point the production of PTH begins to rise, acting on the part of the kidney that still works. With more PTH in the circulation, the phosphorus falls again, returning to normal levels. However, the bone is already beginning to suffer. Even in the early stages of kidney disease, when creatinine is still low, The patient already begins to have bone disease because he needs higher PTH levels to keep the phosphorus controlled.
Therefore, phosphorus control should be initiated in the early stages of renal failure when the function is below 60 ml/min. Few doctors know how to do this type of control, which makes early referral to the nephrologist important in the treatment of bone disease of renal failure.
How to control phosphorus?
The patient who can no longer eliminate the phosphorus correctly through the urine, should then reduce its consumption through a diet low in phosphorus.
You should avoid foods rich in phosphorus, which are:
Milk and its derivatives, including ice cream and yogurt
Foods made with whole wheat flour (bread, cakes, biscuits, toast)
Cola-based soft drinks (Coca-Cola and Pepsi)
Beer
Sardine
Sausages, hams, sausages...
There are medications that inhibit intestinal absorption of dietary phosphorus. They are the so-called pickups or phosphorus chelators. The most common are:
Aluminum hydroxide (disused due to aluminum toxicity in chronic renal)
Calcium carbonate
Calcium acetate
Sevelamer (Renagel or Renvela)
Lantanium carbonate
These substances bind to phosphorus in the intestines, impede their absorption and are eliminated in the faeces. The problem is that only 50% of the phosphorus ingested binds to these chelators. Therefore, regardless of its use, the diet low in phosphorus is essential. Of course, phosphorus chelators only work if taken during meals.
Imagine the following picture: The maximum recommended phosphorus intake for renal patients is 800 mg / day. If a patient does not eat any type of diet and consumes 2600 mg of phosphorus, even if half of it goes out in the stool bound to the chelators, it will still absorb 1300 mg, which is well above the limit.
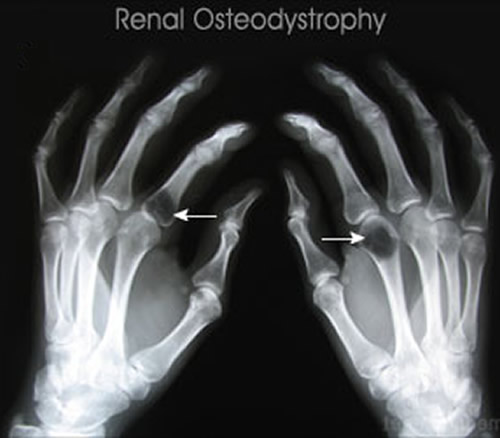
As has been said, elevated phosphorus in the blood (hyperphosphatemia) causes elevated PTH, which, together with insufficient vitamin D causes severe bone damage. This disease is called renal osteodystrophy.
However, this is not the only problem of excess phosphorus.
When in excess, the blood phosphorus binds to the circulating calcium, forming the calcium phosphate, an insoluble substance that precipitates in the blood vessels. The end result is the calcification of these vessels, obstructing the flow of blood. It is no wonder that the main causes of death in patients with renal insufficiency are cardiovascular diseases such as heart attack and stroke.
Excess phosphorus can also precipitate in the skin leading to an intense and diffuse itchiness.
Phosphorus levels in patients with renal failure outside of dialysis should be between 2.7 and 4.6 mg/dl. In patients on dialysis, the values should be between 3.5 and 5.5 mg/dl.
PTH levels in non-dialysis patients should be between 70 and 110 pg/mL. On dialysis the values are 150 and 300 pg/mL.