Acute Pulmonary Edema - Causes, Symptoms and Treatment
Acute pulmonary edema (APE) is a medical emergency caused by leakage of water from the blood vessels into the lung tissue, making breathing difficult. In this paper we explain the causes, symptoms and treatment of acute pulmonary edema.
The edema of the lung has the same pathophysiologic mechanism as any swelling in the body, occurring whenever there is water leakage from blood vessels into a tissue.
Contrary to what one might imagine, our blood vessels tubes are not waterproof, they do have pores that allow the entry and exit of cells, bacteria, proteins and water.
The lung edema occurs primarily through two mechanisms:
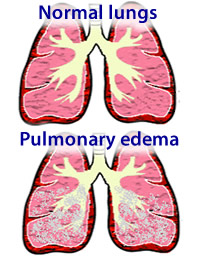
Increased pressure within the blood vessels. When the pressure gets too high within the vessels of the lung, water blood tends to "turn into serum" through pores, accumulating within lung tissue, mainly in the alveoli, which are the structures that perform gas exchange.
Increased vessel permeability. Some diseases, which will be explained below, cause an increase in the pores of blood vessels, making them more permeable, which facilitates the outflow of water.
The most common cause of pulmonary edema is heart failure. We describe simplified cardiopulmonary circulation for this mechanism so that it is easily understandable.
The left side of the heart is responsible for pumping oxygen-rich blood into the body. After nourishing all tissues, blood, now low in oxygen and high in carbon dioxide, it returns to the right side of the heart where it is immediately pumped toward the lungs. In the lungs the blood is oxygenated again and returns to the left side of the heart, where it will be pumped into the rest of the body, restarting the process.
When the left side of the heart becomes weak, it finds it difficult to adequately pump blood to the rest of the body. As the left side of the heart is responsible for pumping blood from the lungs and when the heart pump fails, there is a jam, causing an accumulation of blood in the pulmonary vessels. This congestion causes an increase in blood pressure in pulmonary vessels, favoring leakage of water.
In heart failure pulmonary edema develops slowly unless there is some factor triggering an acute worsening of heart function.
Acute myocardial infarction
The acute myocardial infarction, commonly known as a heart attack, can be caused by pulmonary edema if there is a large area of the heart muscle on the left side of the heart, leading to sudden heart failure. If much of the heart muscle dies, the heart becomes unable to pump blood properly, causing this retention in the lungs. The acute pulmonary edema is one of the possible symptoms of a heart attack.
Hypertensive crisis
The increase in pressure tends to be a frequent cause of acute pulmonary edema, especially in patients who already have some degree of heart failure.
In normal situations the patient's heart with moderate heart failure may still be able to pump blood properly. However, just a sudden elevation in blood pressure is enough for an increase in resistance to blood flow, requiring further work of the heart muscle. Some patients do not have a heart able to work against high blood pressure, which leads to pulmonary congestion.
Disease of the heart valves
If a patient has a disease of the left heart valves, i.e., aortic or mitral valve, it may be difficult for the heart to pump blood through them. Aortic stenosis and mitral valve are lesions that disrupt its opening. If the heart valve does not open properly, blood cannot be drained there through, causing congestion.
Renal failure
Renal failure
Renal failure leads to accumulation of water and salt in the body, causing an increase in the volume of liquid within the vessels. In some cases, especially if the patient does not urinate in appropriate volumes, the quantity of liquid trapped in the vessels becomes so large that it starts to overflow, causing edema and pulmonary edema.
Infections
Some lung infections, particularly those of viral origin, may cause a frame of intense pulmonary inflammation, leading to increased permeability of vessels and subsequent leakage of fluid into the lung. This table is usually called ARDS or SARS (severe acute respiratory distress syndrome).
The high altitude
High altitude
Some people when exposed to altitudes above 2500 meters can develop pulmonary edema. The cause is unknown, but it is believed that there are changes in the pulmonary microvasculature favoring fluid leakage at high altitudes.
The risk factors for this type of acute pulmonary edema are:
Leaving sea level and reaching high altitudes in a short time
Practicing physical exertion at high altitudes without giving proper acclimatization time
Traveling to high altitudes already having a history of heart problems
Excessive intake of alcohol without adequate time for acclimatization to altitude
Drugs
The use of some drugs, such as heroin or cocaine, can cause severe pulmonary inflammation, leading to increased permeability of vessels and subsequent pulmonary edema.
Aspirin intoxication (ASA) can also lead to the development of acute pulmonary edema.
Neurological injury
Some patients with severe neurological injury, such as head trauma, brain surgery, convulsions, cerebral hemorrhage, etc. may develop pulmonary edema. The edema arises from changes in pulmonary hemodynamics, with increased pressure and permeability in the pulmonary vessels.
Depending on the cause, the picture of pulmonary edema may develop slowly or suddenly, the latter called acute pulmonary edema.
Intolerance to exertion
In patients accumulating fluid in the lungs slowly and gradually, the symptoms of pulmonary edema begin with intolerance to exertion, fatigue (even at rest), shortness of breath when lying down, no need to use at least two pillows to sleep, swelling in the feet and ankles and wheezing. This frame is typical in patients with heart failure who have gradual worsening of heart function and progressive pulmonary congestion.
If this same patient described above presents a factor of decompensation of their heart failure, such as a heart attack, a hypertensive crisis or even a serious infection, heart suddenly becomes unable to adequately pump blood to the body, and there is a framework of acute fluid retention in the lungs. In this case the symptoms of acute pulmonary edema are severe: shortness of breath, feeling of drowning, agitation, cough with frothy secretions, inability to lie down and tachycardia (racing heart).
The water in the lungs prevents blood oxygenation and works basically like a drowning. The acute pulmonary edema is a medical emergency and if not treated in time, will definitely lead to cardiac arrest.
The first step in the treatment of acute pulmonary edema is to provide oxygen to the patient. Usually the patient arrives at the emergency department in hypoxemia, or with low levels of blood oxygenation. In some cases pulmonary edema is so severe and oxygenation is so low, that the patient needs to be intubated and connected to a mechanical ventilator to stay alive.
The goal of treatment is to remove water from the lungs. If the patient can urinate, diuretics are administered intravenously to take swift action. Lowered blood pressure is also important to facilitate the work of the heart, so usually vasodilators are used.
If the patient does not urinate or does not respond adequately to diuretics, the option is the urgent hemodialysis, a method capable of removing up to a quart of water from the lungs in just 20-30 minutes.