Abdominal Aortic Aneurysm - Causes, Symptoms and Treatment
The aneurysm is a dilatation in a segment of an artery, which arises from a fragility of the wall of the artery. Having an aneurysm is always a risk because an artery with a weak and dilated wall is more likely to rupture, causing bulky bleeding.
The aortic aneurysm, the largest and most caliber artery in our body, occurs when a region of this long blood vessel becomes weaker, dilating due to the immense pressure exerted by the blood inside the arteries.
In this article we will explain the abdominal aortic aneurysm, that is, the aneurysms that arise in the segment of the aortic artery located in the region of the abdomen. Aneurysms of the thoracic aorta will be addressed in a separate text.
Aneurysms are defined as a focal dilatation in an artery, with an increase of at least 50% of the normal diameter. Example: 3 cm region in an artery that is 2 cm in diameter.
Aneurysms arise when the wall of an artery is diseased and weakened. The arteries deal with very high blood pressures and must have strong, elastic walls so they do not sag, even when there is a large increase in blood pressure. If a segment of an artery for some reason becomes weaker, the blood pressure will slowly cause a dilation in this region, and may eventually reach its limit of expandability and rupture.
As the arteries carry large volumes of blood under high pressure, the rupture of one of these vessels usually causes intense hemorrhage and a high risk of death. The greater the diameter of an aneurysm, the greater the risk of rupture.
The aortic artery is the largest and most caliber artery in our body. The aorta is born out of the left ventricle of the heart, meaning that it is the first blood vessel to receive blood pumped from the heart. All the blood of the organism must pass through the aorta artery before it is distributed to the rest of the body.
Soon after leaving the heart, the aorta makes a great curve, called the aortic arch, and releases its first branches, which will carry blood to the upper limbs and to the head. The aorta then proceeds towards the lower part of the body, traversing the entire thorax and abdomen.
As the aorta goes down, its diameter becomes progressively smaller. It is born at the exit of the left ventricle with about 3.5 cm in diameter, decreases to 2.5 cm after the end of the aortic arch and presents about 1.5 cm in the segment already below the kidneys.
As the aorta descends, dozens of branches are being tossed to nourish tissues and organs along the body, including the intestines, stomach, spleen, liver, kidneys, etc. In the lower part of the abdomen, the aortic artery bifurcates, transforming into the iliac arteries, responsible for irrigation of the lower limbs and pelvis.
Technically, the abdominal aorta begins shortly after the passage of the artery through the diaphragm, a structure that physically separates the chest from the abdomen.
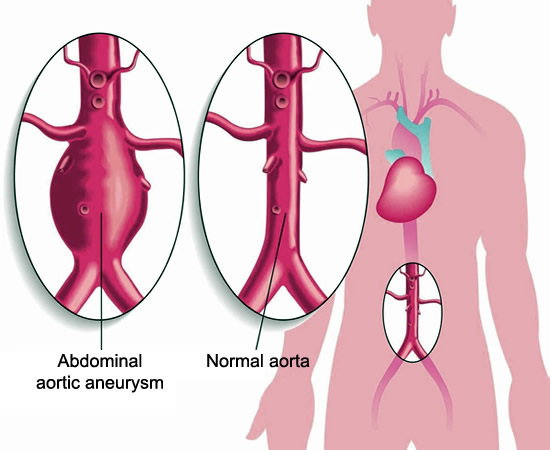
Most aortic artery aneurysms arise in the abdominal aorta. Of these, more than 90% are located below the level of the renal arteries, as in the illustration above.
The main risk factor for an aortic aneurysm is the age of the patient. Abdominal aortic aneurysms are uncommon in people under 50 years of age. Its incidence begins to rise from 60 years, reaching a peak in individuals between 75 and 80 years of age. About 10% of the population over 60 years have an abdominal aortic aneurysm; however, most of these are small aneurysms with a low risk of rupture.
In addition to age, there are other factors that increase a person's risk of developing an abdominal aortic aneurysm:
Cigarette smoking significantly increases the risk of aortic aneurysms. More than 75% of large aneurysms occur in smokers. The risk is directly related to the amount and time of smoking.
Gender: Men are four to six times more likely to develop aneurysms of the aorta than women.
Ethnicity: Caucasians (whites) are the group with the highest risk of developing aortic aneurysms.
Family history: There is a clear genetic association in the risk of developing an aortic aneurysm. Those who have a close relative with a history of abdominal aortic aneurysm present a greater risk of having it.
Aneurysms in other arteries: patients who have aneurysms in other arteries of the body, especially in the lower limbs, are at high risk of also developing aneurysms in the abdominal aorta.
Some diseases are also more related to the development of abdominal aortic aneurysms, among them we can mention:
It should be noted that not every abdominal aortic aneurysm is at risk of rupture in the short term. Two factors should always be observed when assessing the risk of an aneurysm rupture: size and speed of growth.
Studies have shown that aneurysms with a diameter of less than 4 cm are not at risk of rupture and aneurysms up to 5.5 cm are very low risk. The chances of an abdominal aortic aneurysm breaking in the 1-year interval are as follows:
0% for aneurysms smaller than 4.0 cm in diameter
0.5 to 5% for aneurysms between 4.0-4.9 cm in diameter
3 to 15% for aneurysms between 5.0-5.9 cm in diameter
10 to 20% for aneurysms between 6.0-6.9 cm in diameter
20 to 40% for aneurysms between 7.0-7.9 cm in diameter
30 to 50% for aneurysms starting at 8.0 cm in diameter
Regarding the speed of expansion of the aneurysms, we know that those that grow about 0.5 cm in six months also have a high risk of rupture.
Most abdominal aortic aneurysms are small and do not cause any symptoms. In fact, most people who have an aneurysm do not know they have them. Many aortic aneurysms are discovered by accident while performing an ultrasound or computed tomography of the abdomen requested by some other medical reason.
As the aneurysm grows, some signs and symptoms may begin to be noticeable. About 30% of aneurysms are discovered after detecting a small pulsating mass near the umbilicus. Some aneurysms can cause pain in the abdomen or back, and end up being diagnosed during the investigation of this pain.
Unfortunately, most aneurysms grow without causing symptoms and the patient can only discover the lesion in the aorta when it breaks. The rupture of an abdominal aortic aneurysm usually causes intense abdominal pain and rapidly evolves into circulatory shock due to the great blood loss. About 65% of patients die before they even get to the hospital. In some cases, however, bleeding from a ruptured aneurysm may be temporarily contained by some intra-abdominal structures, giving the patient time to receive medical attention.
Correction of an abdominal aortic aneurysm is done through surgery. Once the rupture has occurred, the success rate is much lower than if the surgery had been performed electively before the rupture. The goal of treatment, therefore, is to correct the aneurysm before its rupture.
But all abdominal aortic aneurysms need to be operated?
The answer is no. Surgical repair of an aneurysm is a complex surgery and carries risks. Surgery is indicated in cases where the risk of short-term rupture of the aneurysm is greater than the risks of the surgery itself. Therefore, surgery is generally not advisable if you have an aneurysm smaller than 4.0 cm in diameter. In these cases the patient should only perform abdominal ultrasonography regularly (every 6 months) to confirm that the aneurysm is stable, without growth and without risk of rupture in the short term.
Patients with an aneurysm between 4.0 and 5.5 cm should discuss their options with their physician. The best solution will depend on the surgical risk of the patient and the risk of short-term rupture of the aneurysm. In these cases, the characteristics that influence the decision include:
Surgical risk. Patients with multiple diseases, whose surgical risk is high, should preferably avoid surgery.
In patients where surgery is indicated, there are two surgical options.
Traditional surgery consists of removal of the entire aneurysmal segment and replacement by a graft (prosthesis). This is a large operation and, as already mentioned, carries some risks. However, it is successful in most cases. The graft usually works well for the rest of the patient's life.
The traditional surgery takes from 4 to 6 hours and is done under general anesthesia. After surgery, the patient is taken to the intensive care unit for monitoring. Patients are usually able to be discharged after four to seven days, and can resume their normal activities in about four to six weeks.
A newer, less invasive surgical procedure called endovascular repair has been successful in repairing aortic aneurysms. In this technique, a graft (stent) is taken to the aneurysm site by catheterization of an artery of the lower limbs, usually the femoral artery. The technique is similar to the implantation of stents in cardiac catheterization.
The endovascular technique is safer because it is not exactly a surgery. The procedure usually takes 1 to 3 hours and patients usually leave the hospital within 1 or 2 days. Normal activities can be resumed for 2 to 6 weeks.
But not everything is perfect. There is less experience, less data on long-term outcomes and the success rate of the endovascular technique is not as high as that of open surgery. In addition, over time, the stent may be removed, forcing a new procedure.
Currently, stents are more indicated in elderly patients with multiple medical conditions that increase the risk of conventional surgery.