Botulism - Causes, Symptoms, Diagnosis and Treatment
Botulism is an uncommon disease, potentially fatal, resulting from the action of a neurotoxin (toxin that attacks the neurons) produced by the bacterium Clostridium botulinum. The botulinum neurotoxin is one of the most lethal poisons we know.
Botulism is a disease, which is not contagious (it is not transmissible between people), caused by the action of toxins produced by the bacterium Clostridium botulinum.
Botulism is rare but may occur anywhere in the world. Although it is less common, it is an important disease because infected patients have high mortality and need to start treatment quickly. Botulism is therefore a medical emergency.
The disease is not caused directly by bacteria, but by neurotoxins produced by it. Botulism is an illness of sudden onset with predominantly neurological impairment, characterized by progressive motor paralysis. The main mode of transmission is through poorly maintained food (it will be explained later).
Due to the severity of the disease and the possibility of the occurrence of multiple cases resulting from ingestion of contaminated food, reporting a single case is to be considered as the existence of an outbreak of botulism.
Clostridium botulinum is a bacterium that can be present anywhere, but is most easily found in soil, sediments of lakes and seas, in the intestines of fish and shellfish, agricultural products, honey or on the surfaces of fruits, vegetables and other foods.
Clostridium botulinum is the environment in the form of spores which are very heat resistant and can survive temperatures up to 100°C for five hours or more. The spores are only destroyed by heating above 120°C for at least 15 minutes. When environmental conditions are present, the spores can germinate and develop into a vegetative form, which is the active form of bacteria that can multiply and produce toxins. The best conditions for survival of Clostridium botulinum are:
Low oxygen exposure
Locations of low acidity
Temperature between 25 and 37°C. However, some strains can grow at temperatures as low as 4°C
Some foods, especially preserved, if not properly handled and stored, can become an excellent medium for the growth of Clostridium botulinum.
Some strains of this bacterium produce enzymes that denature and "spoil" the food inhabited by them, leaving them with unpleasant smell and appearance. However, there are strains of Clostridium botulinum that can colonize foods without causing major changes in their appearance, being difficult to suspect that they are contaminated.
Clostridium is a bacterium that causes disease through production of toxins. In the case of the Clostridium botulinum toxin it is a neurotoxin that attacks peripheral nerves, impeding its normal functioning.
Botulinum neurotoxin produced by Clostridium botulinum is one of the most potent poisons we know. Just as a comparison, the cyanide is lethal in mice with a dose of 10,000 micrograms per kilogram. Whereas botulinum toxin can kill with just 0.0003 micrograms per kilogram.
Eight botulinum toxins are known: types A, B, C1, C2, D, E, F and G, of which the type A, B and E are the most toxic to humans. The forms F and G can also cause disease, but it is rare.
Botulinum toxin has no smell or taste, it is not possible to know beforehand if the food eaten is contaminated. The toxins cause illness if ingested because they can withstand stomach acid and natural enzymes in the digestive process. However, unlike bacteria, which can resist higher temperatures in the form of spores, toxin is usually inactivated when exposed to temperatures higher than 80°C for at least 10 minutes.
The toxin absorbed from the gastrointestinal tract reaches the bloodstream and travels to the nerves, where it acts by blocking the action of neurotransmitters responsible for muscle movement, resulting in flaccid paralysis of muscles.
There are basically three ways to acquire botulism: foodborne botulism, wound botulism, intestinal botulism (also called infant botulism).
Wound botulism
This form of transmission is acquired through contamination of wounds with Clostridium botulinum from the environment, usually ground. The main entrance doors are limb ulcers, traumatic injuries or surgical wounds. Botulism can also be transmitted through injecting drugs such as heroin, or inhalable drugs, such as cocaine.
Foodborne botulism
It occurs when the patient eats food contaminated with botulinum toxin. Such contamination usually occurs with improperly preserved foods. Most involved are: canned vegetables, like palm and pickles, cooked meat products, cut and smoked by hand, such as sausage, ham and canned meat, smoked fish, salted and fermented cheeses and artisanal honey. Botulism can also occur in industrialized canned foods.
Intestinal botulism (infant botulism)
It usually occurs in children aged between 1 week and 1 year (most cases between 3 and 26 weeks) and results from ingestion of spores of Clostridium botulinum present in food or soil.
This form is common in honey, which is often contaminated with Clostridium botulinum. However, the large amount of sugar in the honey prevents the transformation of spores to vegetative form, and there is therefore, no toxin production. After ingestion, having reached the intestines, the spores are able to be more active, going to multiply and produce toxins.
Young children still do not have a flora of bacteria in the gut, which can protect them against the invasion of Clostridium botulinum, allowing it to easily set up and produce toxins to pass directly into the intestine.
This form does not usually affect healthy adults, because the spores are unable to fix the intestines. However, adults with diseases of the intestines can also acquire this type of botulism. Risk factors tend to be: intestinal surgery, Crohn's disease or antibiotics for a long time, which causes the elimination of natural intestinal flora.
The incubation period of botulism varies according to the type of transmission. In foodborne botulism, as enzymes are ready in foods, the incubation period is usually short, in most cases between 12 and 36 hours but may range from 2 hours to 10 days depending on the amount of toxins. In wound botulism the average incubation time is 7 days but may vary from 4 to 21 days. In infant botulism there is no precise information about the incubation period, it is often difficult to identify when the spores were ingested. Generally, this period is longer than in foodborne botulism, since the ingested spores must first attach to the intestine, and then move to vegetative form, and only then begin producing neurotoxins.
a. Symptoms of foodborne botulism
Foodborne botulism
Botulism is a progressive illness of sudden onset, characterized by gastrointestinal and neurological symptoms. The gastrointestinal manifestations usually occur early in the frame, but this is not mandatory. The most common symptoms are nausea, vomiting, diarrhea and abdominal pain.
Neurological manifestations tend to be the most important, characterized by muscle paralysis that affects the cranial nerves and initially goes down for the rest of the body. The picture is quite similar to Guillain Barre syndrome, the difference is that botulism begins in the head and progresses downward, whereas in GB muscle paralysis starts in the legs and moves up.
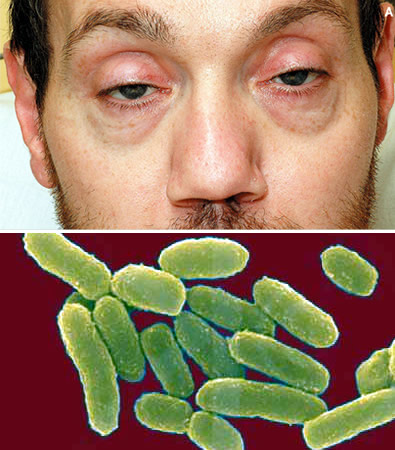
Neurological symptoms of botulism usually begin with blurred or double vision, paralysis of the eyelids, dilated pupils and limitation of eye movements.
From the eyes the disease is reaching the rest of the head, affecting speech, chewing, swallowing capacity and tongue movements. The next step is the affection of the neck muscles, preventing the patient to sustain the weight of the head.
When it comes to the body, paralysis can compromise the functioning of the diaphragm muscles responsible for breathing, leading the patient to acute respiratory failure requiring mechanical ventilation (respirator).
Along with the trunk, the paralysis usually also affects the arms and then the legs and abdomen, causing the patient to a flaccid tetraplegia (flaccid paralysis of four limbs). Dry mouth, paralysis of the intestines, urinary retention and hypotension are also common symptoms.
As the neurotoxin attacks only the muscle nerves there is no impairment of sensitivity, i.e. the patient feels everything, he/she just cannot move the muscles. Blindness is also present while the individual is conscious the whole time.
Symptoms of botulism usually progress for a week or two, leveling off for another 2 weeks before beginning a slow recovery phase, which typically lasts up to 3 months. In more severe cases complete recovery may take up to a year.
The severity depends on the amount and type of toxin ingested (A and B tend to be the most aggressive). The severity of botulism can range from mild, with intestinal symptoms and only minimal involvement of the cranial nerves, to a fulminant disease, and death in just 24 hours. The respiratory paralysis occurs in 30-50% of cases. Hospitalization is usually for at least 1 month; however, there may be patients who need to stay in hospital for up to 3 months.
b. Symptoms of wound botulism
The clinical picture of wound botulism is almost equal to the foodborne botulism, except for the longest incubation period and absence of gastrointestinal symptoms. Fever may also occur, but it is usually due to infection of the wound and not the direct action of toxins.
c. Symptoms of infant botulism (intestinal botulism)
Infant botulism attacks babies and usually manifests itself with constipation and irritability, which progress to neurological signs, such as difficulty controlling the movements of the head, weak sucking, gagging, weak cry, prostration and bilateral paralysis, which can cause breathing failure.
The severity of infant botulism is also variable, and there may be only mild cases characterized by feeding difficulties and mild muscle weakness to severe cases with sudden infant death.
The diagnosis of botulism is usually made in the isolation of toxin in feces or blood. The research of bacterium Clostridium botulinum itself in stool is also possible. In cases of wound botulism, it's no use of examining the stool, you need to look for bacteria in the wound or blood.
The earlier material is gathered, the greater is the chance of finding toxins or bacteria.
For public health issues it is also important to search for the toxin or spores in food ingested by the patient recently, especially with the highest risk, such as honey, canned food, canned fish poorly maintained, etc.. In recent years, worldwide, there were reported cases of botulism caused by cheese, canned sardines, pepper, pickled cabbage, mortadella, tofu, pork, pickled olives and eggplant.
Every patient with suspected botulism should immediately be hospitalized for monitoring respiratory function.
There is an antidote to botulinum toxin, called serum antibotulinico (SAB). This treatment, however, only works against the toxin circulating in blood, or from those that have not yet settled to the nerves. Therefore, the earlier the serum antibotulinico starts working, the greater is its effectiveness. Antibiotics, such as penicillin, can be used in the cases of botulism wound, helping to eliminate any bacteria that are reproducing in the lesions. In patients allergic to penicillin the Metronidazole is an option.
In general, most patients who receive medical care and respiratory care early have a complete or nearly complete recovery and can resume exercising any kind of activity. But patients with severe disease and/or delay in starting treatment may remain with sequels.
Botulism does not provide permanent immunization. The same person may have botulism more than once in a lifetime.