Cardiac catheterization is a medical procedure used to diagnose and treat, when necessary, cases of obstruction of the coronary arteries, which are the arteries that nourish the heart muscle. Untreated obstruction of the coronary arteries results in acute myocardial infarction.
Cardiac ischemic disease is caused by an obstruction of one or more coronary arteries, preventing the adequate flow of blood to the heart muscle, called the myocardium. Like any tissue in our body, the myocardium when deprived of its blood supply goes into ischemia and may undergo necrosis, characterizing myocardial infarction. As the basic mechanism of this disease is a coronary artery obstruction, the treatment consists of unclogging it as soon as possible, preventing an ischemia from becoming an infarction.
In order to make learning about ischemic heart disease more complete, we also suggest reading our other texts on coronary disease, in which we address in detail the symptoms, causes and prevention of angina and infarction.
What is cardiac catheterization? What is coronariography?
We will start with cardiac catheterization, also known as coronary angiography or coronary angiography. Let's use figures and videos to make the explanation simpler.
Cardiac catheterization is an angiography, a radiological examination in which we can analyze the blood vessels. Exam theory is simple:
1. We chose a vessel to be studied, for example, the coronary arteries.
2. Through a puncture of the femoral artery (that is in the thigh), or in the radial artery (in the arm), we introduce a long catheter through the aorta artery until arriving to the heart, in the point where the coronary arteries are born.
3. Through this catheter, small volumes of radiopaque venous contrast are then administered, causing the same to pass through the coronary arteries to "paint" them in order to make them visible through an x-ray examination. simple radiography, on coronary angiography, we obtain several consecutive images, making a film of all the passage of the contrast through the arteries.
See the video below to better understand the explanation. In this film it is possible to see the contrast being delivered by the catheter directly into the coronary arteries. There are 4 consecutive administrations presented in the video provided below.
If one of the arteries is filled with cholesterol plaques that block the passage of blood, they are also blocking the passage of contrast, and this is easily noticeable during angiography, as can be seen in the image below. The arrow shows the exact location where there is an obstruction of the vessel. Note that the obstruction point has almost no contrast inside.
Coronary angiography is currently the best method for the diagnosis of coronary artery obstructions.
Once the coronary angiography is done, we can decide what strategy we will adopt with the patient. If the vessels are without signs of obstruction, the examination is terminated and the catheter is withdrawn. On the other hand, if angiography points to obstructive coronary lesions, it becomes necessary to unclog them. If the lesions are very severe and multiple, the alternative is bypass surgery. If only one or at most two branches of the coronary arteries are diseased, angioplasty can be performed.
Angioplasty is a non-surgical procedure in which it is possible to unclog arteries with poor blood flow caused by cholesterol plaques on your wall. Angioplasty can be done in various arteries of the body, but in this text we will speak only of coronary angioplasty.
Angioplasty is performed immediately after coronary angiography. Once the obstructed artery is identified, a special balloon for angioplasty is inserted deflated by the catheter that is now located inside the diseased coronary artery. Upon reaching the plate site, this balloon is inflated to a pressure of 20 atmospheres, making it incredibly hard, capable of literally crushing the fat plate, reopening the lumen of the artery and allowing blood flow to return to normal.
Look at the image below showing a coronary angiography done before the balloon angioplasty and another done after the angioplasty. Note that before, there was a failure in the filling of the artery by contrast, indicating an obstruction of blood flow. After the plaque was destroyed by the balloon, the contrast began to follow its path without restrictions.
The term cardiac catheterization encompasses two different procedures: diagnostic catheterization, which is simple coronary angiography, and therapeutic catheterization, which includes angioplasty. When the patient only says that he has had a cardiac catheterization, it is necessary to complete the information saying whether or not angioplasty was done, so that we can know exactly what type of procedure he underwent.
Balloon angioplasty has excellent short-term results, with success rates above 90% for resolution of pain and restoration of blood flow. However, in the medium / long term the reobstruction of the coronary artery is very common. About 30% of patients will have their arteries plugged again within 6 months. Therefore, in addition to balloon angioplasty, an additional procedure is necessary to ensure a prolonged patency of the coronary arteries: implantation of a stent.
What is angioplasty with stent?
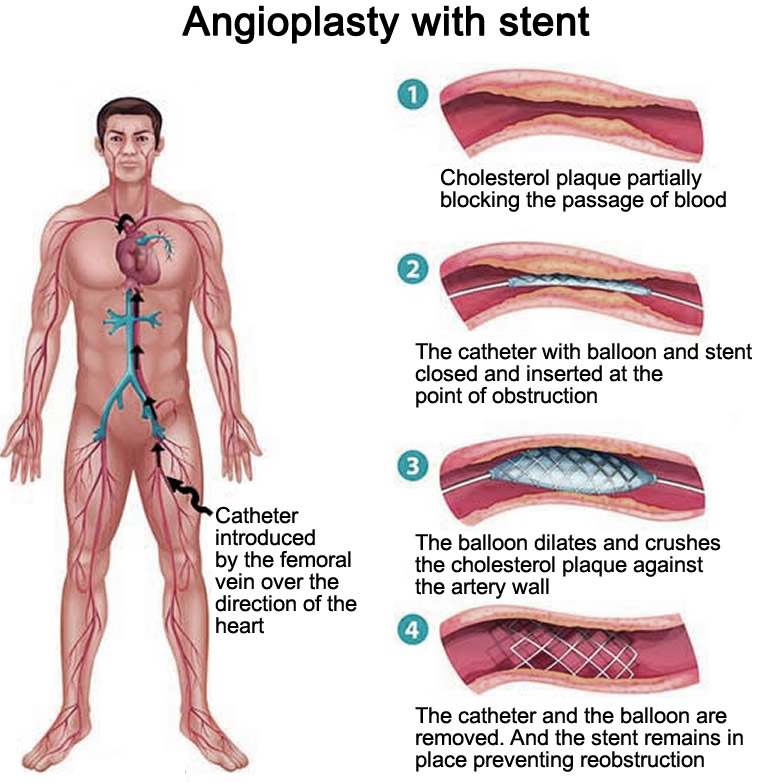
The stent is a cylindrical, expandable metal prosthesis that is implanted shortly after balloon angioplasty in order to decrease the chance of the coronary artery being again obstructed by atherosclerosis over time. The stent implantation process is the same as for angioplasty. See the illustration on the left.
Currently, there is practically no more angioplasty without the placement of a stent due to a large difference of results between the two procedures.
After stent angioplasty
Stent angioplasty is a reasonably simple procedure and the patient is usually discharged the next day, and is hospitalized overnight for observation only.
At the end of the procedure, the catheter is removed and the patient should lie down for a few hours with compression on the femoral artery to prevent bruising at the catheter insertion site.
The stent patient usually needs to take medications that inhibit the action of platelets to inhibit clot formation and stent thrombosis. Aspirin and clopidogrel (Plavix) are the two most prescribed drugs.
The stent modern are composed of materials that do not contraindicate performing nuclear magnetic resonance (NMR), unlike the older prostheses. If you have a stent and need to have an MRI, ask your cardiologist if your stent is safe, called by the manufacturer as "MR safe".
There is no invasive medical procedure without risk. Complications of cardiac catheterization are uncommon if all precautions are taken, but there is always a small risk of problems. Among the possible complications, we can mention:
Allergy to the venous contract
Bruising and bleeding at the puncture site
Embolization of thrombus fragments after angioplasty
On this last complication, we find it important to spend a few lines.
Acute renal failure after cardiac catheterization
Most of the venous contrasts used for radiological exams are toxic to the kidneys, causing a temporary drop in the rate of blood filtration.
People with healthy kidneys do not have complications, because even if they lose half of their kidney function for a few days, they can survive well with the remaining 50% of function. People who already have kidney disease, however, do not have this reserve to tolerate large falls in their renal function, with the occurrence of transient acute renal failure, with an average duration of 7 days.
Cardiac catheterization in a patient with a previous diagnosis of chronic renal failure should be done very carefully, and if possible with the help of a nephrologist, because the risk of deterioration of renal function in the first 48 hours after contrast is immense. Kidney toxicity may be so severe that some patients may require hemodialysis for a few days.
The highest risk for contrast nephrotoxicity occurs in patients who have:
Blood creatinine value before examination greater than 1.5 mg/dl