Multiple Sclerosis - Causes, Symptoms, Diagnosis and Treatment
Multiple sclerosis is a disease of probable autoimmune origin in which our body inappropriately produces antibodies against structures of our nerves, leading to inflammation and destruction of them.
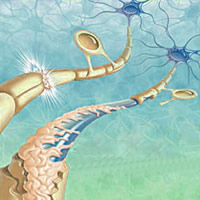
Multiple sclerosis is a neurological disease that occurs through the destruction of myelin, the substance that covers nerves. Therefore, to understand the multiple sclerosis you must learn what the myelin sheath is.
All our nervous system communicates through electrical impulses. For example, we are able to move our hand because our nervous system is able to send an electrical impulse, leaving the brain through the spinal walks, going to the peripheral nerves and reaches the muscles of the hand, giving order for them to move. Impulses can also follow the reverse path. We are able to perceive temperature, touch, pressure, pain, etc. because the nerve endings in the skin capture these stimuli, sending them to the peripheral nerves, spinal cord and ultimately the brain, where they are interpreted.
These electrical signals coming to and from the brain need to be transported between neurons. The leitmotif of the neurons responsible for this connection is called the axon, an extension of the neuron itself able to connect one nerve cell to another. Like any electrical wire, axons require insulation, like a wire wrap. The substance that provides this isolation and allows the transmission of electrical impulses is the myelin sheath.
In multiple sclerosis the nerve cells of the brain and spinal cord exhibit their progressive destruction of myelin sheaths, causing the axons lose the ability to carry electrical impulses. The central neurons fail to send and receive electrical stimuli.
Multiple sclerosis is an autoimmune disease caused by destruction of the myelin sheath by our own antibodies. We do not know quite why, but all of a sudden our body starts to treat the myelin sheath as a strange structure, like a virus or bacteria. The immune system then starts attacking the myelin sheath of neurons, progressively destroying it. It is thought that the origin of multiple sclerosis may be related to immune system disorders that arise after some viral diseases, for example, mononucleosis.
Differences between multiple sclerosis and Guillain-Barre
Multiple sclerosis and Guillain-Barre disease are similar, both have an autoimmune origin and both attack the myelin sheath of the nerves. The difference is that the Guillain-Barre the peripheral nervous system (outside spinal nerves) is affected, while in multiple sclerosis it is the nerves of the central nervous system (spinal cord and brain) that undergo demyelination. This slight difference is important in the final diagnosis, since the peripheral nerves have the capacity to regenerate, whereas the axons and neurons in the brain and spinal do not.
Multiple sclerosis usually declares itself first between the age of 20 and 40. It is twice as common in women as in men, and three times more common in people who have a family member affected by the disease. Multiple sclerosis occurs more frequently in Caucasians (whites) than in people of Asian or African descent.
Apparently, one of the risk factors for the onset of multiple sclerosis is infection by the Epstein Barr virus, which causes mononucleosis. It is thought that the virus may have similar proteins of the myelin sheath, causing the antibodies have difficulty distinguishing between them. Importantly, the vast majority of patients who had contact with the Epstein Barr virus do not develop multiple sclerosis, suggesting that more than one factor are necessary for the emergence of the disease.
Patients with other autoimmune diseases such as Hashimoto's thyroiditis, diabetes mellitus type 1 or Crohn's disease also exhibit increased risk of developing multiple sclerosis.
The signs and symptoms of multiple sclerosis depend on which parts of the nervous system are affected. There is a typical symptom that closes the diagnosis of multiple sclerosis, but some of them are very suggestive:
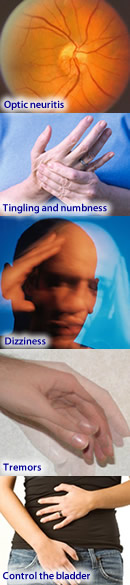
- Optic neuritis: typically presents as an acute pain in one eye, which worsens with eye movement. This pain usually comes associated with varying degrees of vision loss, usually in the center of the visual field. The patient may also experience blurred or double vision. Nystagmus (discrete involuntary eye movement) is a common finding.
The involvement of both eyes at the same time is unusual in multiple sclerosis and it usually indicates other neurological disease.
- Sensory symptoms: tingling and numbness, especially in the limbs, occurring on one side of the body at a time, are very common symptoms of multiple sclerosis and appear in almost 100% of cases over the course of the disease.
- Lhermitte Phenomenon: electric shock feelings radiating through your spine, triggered by movements of the head and neck is called Lhermitte's phenomenon. It is a typical symptom of MS, but may also occur in other neurological diseases.
- Dizziness and vertigo: up to 50% of patients with MS may experience dizziness. This symptom usually appears in patients with involvement of the face by the disease, such as numbness or ocular and auditory alterations.
- Motor symptoms: tremors, changes in gait, decreased muscle strength and paralysis of the limbs occur by injury to the spinal neurons. The loss of strength is initially unilateral but becomes bilateral in advanced stages. The involvement of the lower limbs is typically more intense than in the upper limbs.
- The inability to control the bladder and bowels: a lesion of the spinal nerves and muscle weakness in the lower limbs, it can also cause a loss of control of the anal sphincter and bladder, causing urinary incontinence and fecal incontinence.
Multiple sclerosis manifests alternating periods with remissions attacks. The patient has acute symptoms that last for days to weeks, and then disappear without consequences. The patient remains asymptomatic until a second attack, which also disappears. As the attacks accumulate, they become increasingly aggressive and complications keep adding up, so that the patient will become progressively worse after each exacerbation.
Patients of 30 to 40 years survive multiple sclerosis. Patients who after 10 or 15 years of disease have little or no complications are those with the best diagnosis, with higher quality of life and time.
Multiple sclerosis may have different presentations among patients. There are some well-known patterns of behavior.
1 - Relapsing remitting multiple sclerosis (RRMS) or remission outbreak
This form of MS is characterized by recurrent episodes of sudden onset, but short-lived, followed by complete recovery (partial or minimal complications). No progression of the disease outbreaks off periods, the patient may be months or years without signs of multiple sclerosis. This pattern of MS is responsible for 85 to 90% of the initial cases. However, most patients with RRMS will eventually enter a phase of progressive disease, named secondary progressive multiple sclerosis (SPMS).
2 - Secondary Progressive Multiple Sclerosis (SPMS)
The secondary progressive MS occurs when there is worsening form remitting multiple sclerosis (RRMS), usually 15 to 20 years after disease onset. In this case the crises become more frequent and the consequences begin to accumulate. The patient can now evolve with worsening symptoms even without acute attacks.
3 - Primary Progressive Multiple Sclerosis (PPMS)
The primary progressive multiple sclerosis is characterized by rapid disease progression from the early stages. The patient may not have outbreaks, but will gradually accumulate symptoms and complications. This type has a worse prognosis and represents about 10 percent of cases. It usually arises in patients who develop MS after 40.
There is no single test to establish the diagnosis of multiple sclerosis. Diagnosis is made through the interpretation of symptoms and completing some tests. The tests commonly used for the elucidation of the frame are the nuclear magnetic resonance of central nervous system, analysis of cerebrospinal fluid obtained by lumbar puncture, and the evoked potential test, which evaluates the body's response to small electrical shock, which stimulates peripheral nerves or muscles of vision.
Unfortunately there is no cure for multiple sclerosis. Since this is a disease of immunological origin, its treatment is based on drugs that act on the immune system. The therapy is divided into treatment in crises and treatment during remission.
Corticosteroids are the most widely used drugs during outbreaks (steroids and prednisone). The treatment is called pulse and consists of the administration of high doses of corticosteroids (usually methylprednisolone) is administered intravenously for 5 days.
In cases of severe outbreak, with poor response to corticosteroids, the attainment of plasmapheresis isindicated, a procedure similar to hemodialysis, used to cleanse the blood from harmful antibodies.
There are drugs to treat patients outside of seizures, sequelae to reduce the occurrence of new outbreaks. This treatment, called disease-modifying, is especially effective in cases of MS relapsing remitting multiple sclerosis (RRMS). It does not cure MS, but greatly improves their prognosis.
The drugs most currently used are interferon beta (Avonex, Betaseron or Rebif) and glatiramer acetate (Copaxone). In Brazil these medicines are distributed free by the government.
In severe cases with poor response to interferon and glatiramer, there is still the option for treatment with natalizumab (Tysabri) or monthly pulse therapy with corticosteroids.