Muscle Soreness Caused by Medications for Cholesterol
The statins are a group of widely used drugs in the treatment of high cholesterol. Among the best known drugs of this group, we can cite simvastatin, rosuvastatin, pravastatin and atorvastatin.
The statins, and are the most effective drugs in the control of cholesterol are also those with the best results in scientific studies on prevention of cardiovascular diseases, and is therefore currently prescribed for tens of millions of people worldwide.
Although being safe and effective drug, about 5% to 10% of patients develop myopathy (muscular injury), characterized clinically by muscle pain, weakness, and / or cramps. Patients treated with high doses are those most at risk.
The muscular origin of complaints are the main side effect of statins and the most common cause of discontinuation of therapy.
In this article we make a review of myopathy caused by statins, addressing your symptoms, risk factors and treatment options.
The role of creatine phosphokinase (CPK or CK)
The severity of a muscle injury is defined not only by the symptoms, which include pain and loss of muscle strength, but also by changes in laboratory tests.
The muscle cells are rich in an enzyme called creatine kinase, best known for CK or CPK acronyms. When there is injury to the muscle tissue of the CK enzyme contained in the muscles spills into the blood, causing the blood to raise CK. While small increases in CK may occur in benign situations, such as after intense physical exertion, high elevations in blood levels are a sign of serious muscle disease.
The reference value of CK usually vary according to each laboratory. In general, the upper limit of normal is around 100-200 U / L. Whenever the value of CK is at least 3 times the normal value, we say that the patient has myonecrosis (muscle cell death).
The severity of myonecrosis usually divided as follows:
Slight muscle injury: CK high 3-9 times normal.
Muscle injury moderate: high CK 10 to 50 times the normal value.
Severe muscle injury: CK high more than 50 times normal.
Therefore, a patient with CK around 400 or 500 U / L has only a slight muscle injury, whereas a patient with CK around 70,000 U / L has a severe and extensive muscle injury. If beyond myonecrosis, the patient also has loss of muscle proteins in the urine, an event called myoglobinuria, we say that he has rhabdomyolysis, a severe condition, which can lead to acute renal failure.
Statins generally cause mild muscle injury, with small elevations of CK values. However, about 1 in every 1,000 patients treated with these drugs can develop moderate or severe muscle injury with rhabdomyolysis.
Statins can cause muscle constellation of symptoms which include discomfort, stiffness, fatigue, increased sensitivity, weakness or cramps. Typically, the symptoms appear after physical exertion, but may also be present even at rest.
The intensity of the symptoms is not always directly related to blood levels of CK. Some patients in pain may have low or even normal levels of CK, while others with mild to moderate complaints can have very high rates. Without the dosage of blood CK not possible to precisely define the degree of muscle damage. Therefore, every patient on statin use that starts muscle pain framework should do a blood test to find out the degree of elevation of CK.
Muscle damage
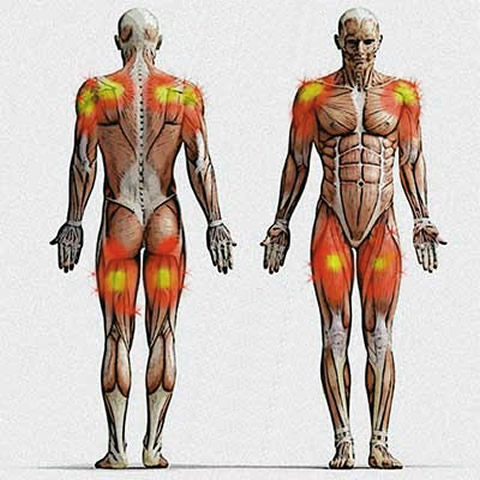
The most common symptoms of myopathy of statins is muscle pain (myalgia), which may or may not be accompanied by strength reduction. Overall, the muscle damage caused by statins causes a picture of pain and weakness, which in the lower limbs affects symmetrically muscles of the pelvis and both thighs, and upper limbs attacks the muscles around the scapula, clavicle and initial portion arms (see illustration).
The loss of muscle strength of myopathy statins can cause the patient has difficulty to lift your arms above your head, rising from a chair or climbing stairs. These symptoms can also be described by the patient as fatigue or tiredness of the members.
Usually, the myopathy statins develops in the first six months of drug therapy, but there are cases of patients who were only develop it after years of drug use.
Complications of myopathy by statins
The muscle damage caused by statins occurs in about 5-10% of users, and even then, the vast majority of cases are mild, without great damage to the patient's health.
Despite the rarity, there may be cases of severe muscle damage caused by statins. The rhabdomyolysis frame is the most dangerous because the muscle protein can block the renal tubules, leading to acute renal failure. It is not uncommon that patients with rhabdomyolysis require treatment with hemodialysis for a few days.
As already mentioned, despite the muscle injury is the most common side effect of statins, it is a problem that only affects some users.
Not yet fully understand the mechanisms by which statins to be toxic to the muscles of certain individuals, but some risk factors are well known, as we will explain below.
Features of statins
The risk of muscle damage not equal for all statins and increases with dose. The pravastatin and fluvastatin appear to be the drugs of this group with the lowest incidence of muscle pain. The dose of 40 mg per day of pravastatin proved to be quite safe and low incidence of muscle injury. The rosuvastatin at a dose of 20 mg / day has also been shown to be safe in the studies, however, doses from 40 mg / day have been identified as responsible for signs of rhabdomyolysis.
Hypothyroidism
Because patients with hypothyroidism often have high cholesterol, it is not uncommon to prescribe statins in this group of patients. The problem is that hypothyroidism alone can cause myopathy, and when combined with a statin, the risk becomes even greater.
The clinical management of hypothyroidism through medicines with levothyroxine reduces the risk of muscle pain.
Patient characteristics
Genetic factors appear to play a role in the genesis of myopathy caused by statins. This is the reason why in the same family is the frequent occurrence of myopathy in more than one person.
Women and people over 60 years are also at increased risk. Other factors that can influence are the frequent consumption of alcoholic beverages, intense physical activity, vitamin D deficiency, dehydration and the presence of kidney or liver disease. People with a history of frequent cramps are also at increased risk of myopathy caused by statins.
Drug interaction
One of the factors that most influence the onset of muscle damage caused by statins is associated with other drugs. The simvastatin and lovastatin are statins suffer most drug interactions can cause myopathy. The atorvastatin to rosuvastatin and pitavastatin can also suffer interaction of some drugs, but with a slightly lower frequency.
Drugs such as: amiodarone, fluconazole, ketoconazole, itraconazole, cyclosporine, gemfibrozil, warfarin, verapamil, amlodipine, erythromycin, clarithromycin, ritonavir, colchicine and niacin materially increase the risk of muscle damage by statins. If possible, this combination should be avoided.
The list provided above is very far from complete, so if you take several medications and has muscle pain by statin, take a look in the package leaflet to see if there are any drug interactions that may be triggering the pain.
What about the patient who has muscle pain by statin
As there is no drug on the market as effective as statins in preventing cardiovascular disease, the decision to suspend or not the treatment should be well thought out. Drugs like ezetimibe are not as effective as statins and should not be regarded as a suitable substitute. The ezetemibe can even be used together with a statin, in order to allow a lower dosage of the latter.
The rare patients who develop severe muscle injury should definitely interrupting the treatment with statins as the health hazard is greater than the potential benefit of the drug. We treat severe myopathy and myopathy with all CK elevation greater than 10 times the reference value (CK greater than 1500-2000 U / L in most laboratories).
In cases that do not fit the concept of severe myopathy, which are actually the majority, there are some strategies that can be implemented.
1. Fix problems
The first point is to identify possible drug interactions that might increase the risk of muscle injury. The combination of a statin with gemfibrozil, although not shown, is still used by some doctors, when the goal is to lower triglyceride levels. If the patient has high cholesterol and triglycerides, and statin alone are not sufficient to control values, the drug with less risk of myopathy is fenofibrate.
In addition to the review of drugs that the patient uses, it is also important an evaluation of thyroid function. In many cases, a simple optimization of treatment of hypothyroidism is sufficient to control muscle pain.
The dosage of vitamin D blood level is also shown. If the values are low, the replacement, which can be done very simply and cheaply, often ease the pain.
2. Changes in statin
With no problems to correct, the next step is to optimize treatment with statins. In patients with high doses of statins, the simple reduction of the daily dose may be sufficient. If necessary, the doctor can associate a drug like ezetimibe, so that the value of LDL cholesterol do not re-up after reducing the statin.
Doses of statins are considered moderate: 40 mg of lovastatin, pravastatin or simvastatin; 20 mg atorvastatin; or 10mg of rosuvastatin. Only patients who have already had a heart attack previously or who have very high risk of heart attack usually have indication for higher doses of statins, usually 40 mg / day of atorvastatin or 20 mg / day of rosuvastatin.
An alternative is the use of statins on alternate days. Rosuvastatin at doses up to 20 mg / day can be taken 3 times a week, which still retains a good action against LDL.
Another option is to switch statin. As mentioned above, pravastatin and fluvastatin usually have a lower incidence of myopathy and can be the solution, especially for patients taking simvastatin or lovastatin, which are the statins that most often cause muscle pain.