Sjögren syndrome is a disease of autoimmune origin, which attacks the glands and organs of our body. This disease affects women, every 10 patients affected, 9 are female.
Sjögren syndrome is a disease of autoimmune origin, that is, it is a disease in which the immune system mistakenly starts attacking cells and tissues of our own body, as if they were dangerous invaders for our health. The immune system produces autoantibodies and stimulates defensive cells, such as lymphocytes, to attack and destroy parts of our own body.
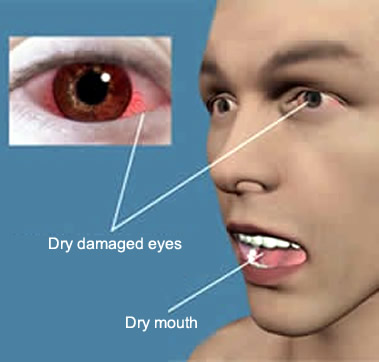
In the specific case of Sjögren syndrome, the main targets are the lacrimal and salivary glands, causing symptoms like eyes and dry mouth. However, the disease may not be restricted to these glands, and other organs such as joints, kidneys, lungs, nerves, skin, liver, pancreas, etc. may also be affected.
As with almost all diseases of autoimmune origin, we do not know exactly why the immune system of these patients suddenly acts in the wrong way, attacking tissues and organs of the body itself.
We know, however, that there is a strong genetic component in its genesis, since patients with Sjögren's syndrome have some genes in common. However, for Sjögren's syndrome to appear, genetic inheritance is not enough, some other unenlightened environmental factors, such as infections by certain viruses or bacteria, appear to be necessary for the immune system of genetically susceptible patients to act in a dangerous way.
About half of patients with Sjögren's syndrome also have another associated autoimmune disease, such as lupus, rheumatoid arthritis, scleroderma, or thyroiditis of Hashimoto. Therefore, having an autoimmune disease is a risk factor for having Sjögren's syndrome, just as having Sjögren's syndrome is a risk factor for having other autoimmune diseases.
We classify as primary Sjögren's syndrome cases in which there is no other associated autoimmune disease. Patients who have Sjögren's syndrome plus another autoimmune disease, such as lupus or rheumatoid arthritis, are considered as having secondary Sjögren's syndrome.
Other important risk factors for Sjögren's syndrome are female sex, since more than 90% of cases occur in women, and age, therefore, although the disease may appear in any age group, it is more common in people above of 40 years.
Xerophthalmia (dry eyes) and xerostomia (dry mouth) are the most typical symptoms of Sjögren's syndrome. However, the disease is usually insidious, with slow progression and with nonspecific symptoms, common to several other rheumatological diseases, especially in the first years, making the correct diagnosis often only after years of investigation.
Inflammation of the lacrimal glands reduces tear production and interferes with eye lubrication, leading to red-eye, dry eyes, burning or foreign body sensation, itching, or blurred vision. Lack of eye lubrication increases the risk of eye infection and corneal injury.
Inflammation of the salivary glands causes reduced saliva production, leading to dry mouth, dry throat, difficulty swallowing, changes in taste, hoarseness, increased incidence of cavities, and injuries to the teeth, gums, tongue and lips. In children, inflammation and swelling of the parotid gland is very common, and the condition can be mistaken for mumps.
In addition to the lacrimal and salivary glands, other areas of the body can also be attacked. Examples are the various areas, where it is possible to have dry cough, sinusitis and rhinitis of lung infections. Inflammation of the vaginal glands, responsible for lubricating the vagina is also common, leading to vaginal dryness, pain during sex and increased frequency of gynecological infections, mainly candidiasis. Tiredness and menstrual changes are also relatively common.
Less common symptoms of Sjögren's syndrome include atrial fibrillation, Raynaud's phenomenon, enlarged lymph nodes, kidney damage, nerve and muscle injuries. A rare complication is inflammation of the blood vessels, called vasculitis, which can damage the tissues of the body that are nourished by these inflamed vessels.
About 5% of patients with Sjögren's syndrome develop non-Hodgkin's lymphoma. This complication usually arises 7 to 10 years after the diagnosis of Sjögren's syndrome.
Sjögren's syndrome is often a difficult disease to diagnose, since the signs and symptoms vary from person to person and may initially be similar to those caused by other diseases such as rheumatoid arthritis, lupus, sarcoidosis, amyloidosis, fibromyalgia, etc. In addition, classic dry mouth and eye symptoms occur in several other diseases, and may also be a side effect of a number of medications. It is not uncommon, therefore, for the patient to only receive the correct diagnosis of Sjögren's syndrome several years after the onset of the first symptoms.
The most suitable specialist to conduct Sjögren's suggestive work is the rheumatologist. There is no single exam that can define the diagnosis with certainty. This is usually done by jointly evaluating signs and symptoms with laboratory tests.
The search for autoantibodies such as FAN, rheumatoid factor, anti-SSA / anti-SSB / It may aid in the diagnosis. However, these autoantibodies have high false positive and false negative rates and are not sufficient for diagnosis without other clinical and laboratory data.
Salivary gland biopsy may be recommended to aid in diagnosis. The procedure is done by removing a small piece of tissue from the inner portion of the lower lip. A gland filled with lymphocytes suggests that it is being attacked by the immune system, which speaks strongly in favor of Sjögren's syndrome.
Eye exams to determine if tear production is normal are also helpful:
Schirmer test: In this test, a small, thin piece of filter paper is inserted gently between the eyelid and the inner corner of the eye. The paper is removed after several minutes, and the humidity is measured. Decreased amount of moisture is characteristic of Sjögren's syndrome, although reduced tear production may also occur with other conditions.
Rose Bengal Test: This test detects lesions in the eyes, mainly in the conjunctiva and cornea, caused by the chronic dryness of the same. It is an eye exam made after dripping an eye drop with a specific dye, called rose bengal. With a special light, the ophthalmologist can detect eye injuries.
There is currently no cure for Sjögren's syndrome. However, the treatments can improve the symptoms and prevent the various complications of the disease.
The treatment aims to reduce the most troublesome symptoms. Dry eyes are treated with artificial tears applied regularly during the day or with night gel applied. Eye drops that reduce inflammation in the tear glands, such as cyclosporin (Restasis), may be used to increase tear production.
To increase salivation, the use of sugarless candy or gum is helpful. Drinking or just wetting your mouth with sips of water during the day is also important to keep it well moisturized. Some patients benefit from the use of drugs that stimulate the flow of saliva, such as pilocarpine (Salagen) or cevimuline (Evoxac).
Since cavities are very common, one should brush one's teeth after any meal. There are already on the market toothpastes aimed at patients with dry mouth. A visit to the dentist should be done 2 times a year.
Hydroxychloroquine is a drug widely used in lupus and rheumatoid arthritis and may be useful in some patients with Sjögren's syndrome and joint pain, muscle and/or dermatological lesions. In patients with systemic disease, affecting several organs, the use of immunosuppressive drugs, such as corticosteroids, azathioprine, methotrexate, rituximab and cyclophosphamide may be necessary.