Polycystic Ovary Syndrome - Symptoms, Causes and Treatment
Polycystic ovary syndrome (PCOS) is a disease characterized by the presence of multiple ovarian cysts, associated with a deregulation of the ovulatory cycle and female hormones.
A cyst is a kind of bag formed by a thin membrane, containing liquid or air inside. It's like those blisters that appear on the skin after a burn or on the foot after wearing an uncomfortable shoe. The cyst is a closed structure, not having direct communication with the tissue in which it is inserted.
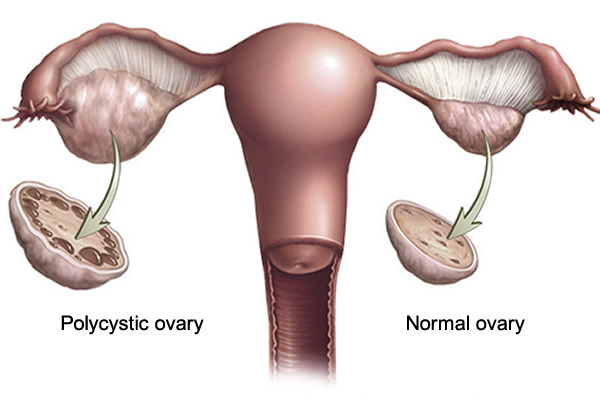
The polycystic ovary, as its name says, is an ovary that develops multiple cysts. To understand why several cysts appear in the ovary one must first know the normal ovulatory cycle. Let's summarize it:
Normal menstrual cycle
The cycle of ovulation occurs through a sequence of events triggered by the brain, ovaries, and uterus, which occur on average once every 28 days (in some women this cycle is larger, in others smaller). The ovulatory cycle is controlled primarily by 4 hormones, two of them FSH and LH, produced by the pituitary gland of the brain, and two others, estrogen and progesterone, produced by the ovaries.
During the first half of the cycle, the brain produces the FSH hormone, which stimulates the ovary to develop several follicles (a type of cyst). In the presence of FSH, the follicles begin to develop, growing and maturing. Seven days after the start of the cycle, several follicles measuring between 9 and 10 millimeters can be detected on ovary ultrasound.
These ovarian follicles begin to produce estrogen. As estrogen levels increase, one of the follicles becomes dominant, developing faster than others, which stop growing and begin to involute. This dominant follicle is who will release the ovum at the time of ovulation.
The peak in estrogen production occurs one day before ovulation. At the time of maximum concentration of estrogen, another hormone from the pituitary gland is released, the LH. We are now right in the middle of the cycle, around the 14th day in cases of 28-day menstrual cycles. 36 hours after LH release, dominant follicle disruption and egg release occur.
After ovulation, the ovary produces estrogen and progesterone, which prepare the uterus for implantation and possible pregnancy. If the egg is not fertilized, it is absorbed and the production of LH, estrogen and progesterone is stopped. Without these hormones, the uterus discolors, thus giving rise to menstruation.
Therefore, menstruation is a sign that the woman ovulated but was not fertilized.
Menstrual cycle in polycystic ovary syndrome
In women with PCOS, follicles that arise due to the action of FSH are unable to grow to a size that would provoke ovulation, so there is no development of a dominant follicle. Without the dominant follicle, there is no ovulation or stimulation for the remaining follicles to involute, with progressive accumulation of them, which is responsible for the polycystic aspect that the ovaries acquire. The absence of ovulation and the constant presence of follicles deregulate the entire cycle of FSH, LH, estrogen and progesterone production. A woman with a polycystic ovary may not ovulate for several cycles, which is easily noticeable because of the irregular nature of her menses.
It is not clear what causes PCOS. It is likely to be the result of the association of genetic factors and environmental factors. About 10% of women have polycystic ovary syndrome to some degree.
The genetic influence is strong. Women with polycystic ovary often have a mother or sister also with the disease. Researchers are still looking for the genes responsible for the disease.
A very common finding in women with polycystic ovarian syndrome is an increase in testosterone levels, the main male hormone. Another common change is insulin resistance. The patient produces insulin normally, but their tissues are resistant to their action, causing a change in blood glucose values.
The polycystic ovary is called syndrome because it has a set of signs and symptoms that may or may not be present. There is a great variability of the symptoms of polycystic ovarian syndrome, the disease being milder in some women and more exuberant in others.
The main characteristics of PCOS are irregular menstruation, which indicates the presence of anovulatory cycles (absence of ovulation), infertility, obesity, enlargement of the hair and acne. Laboratorially it is common to find high levels of glucose in the blood, in some cases (about 10%), high enough to cause diabetes.
Excess testosterone, called hyperandrogenism, is responsible for some of the typical signs and symptoms of polycystic ovary syndrome. Hirsutism is the name given to the presence of hairs in women in places with male characteristics. The hairs usually appear above the upper lip, on the chin, around the nipples and below the navel. Women may also have male-pattern baldness. The excess of male hormones is also responsible for the increase in skin oiliness and the appearance of acne (blackheads and pimples).
Difficulty getting pregnant is very common in women with polycystic ovary. The frequent absence of ovulation is responsible for infertility. Many of the PCOS patients end up needing infertility treatment to get pregnant.
Absence of ovulation and hormonal changes in PCOS increase the risk of developing cancer of the endometrium (the wall that lines the uterus).
Another common finding in polycystic ovarian syndrome is the metabolic syndrome, characterized by being overweight, insulin resistance, high cholesterol and hypertension. Patients with metabolic syndrome are at increased risk of developing cardiovascular disease.
The nigricans acanthosis is an increased pigmentation of the skin in areas of the neck, skin folds, joints or elbows, tonando-blackened, like the image above. It is a typical finding in obese and insulin resistant patients.
Other common changes are sleep apnea and hepatic steatosis.
There is no cure for polycystic ovarian syndrome, but there are effective treatments that can control the symptoms of the disease well.
Treatment is usually directed towards the most exuberant symptoms. In women with hyperandrogenism, the use of birth control pills helps decrease the production of male hormones. Cyproterone acetate, present in Diane, has a good antiandrogenic action.
If there is no response expected after 6 months of the pill, a diuretic called spironolactone can be used because it also has antiandrogenic activity, mainly in the skin, inhibiting hirsutism. Another drug with antiandrogenic effect that can be used is Finasteride. There is a cream called Vaniqa, which can be used on the skin as it inhibits the growth of hairs.
The use of contraceptives, besides the aesthetic part, is also important to regularize the menstrual cycle, reducing the risks of endometrial cancer. The pill also works against acne.
Metformin is an antidiabetic drug widely used in PCOS as it helps control insulin resistance by adjusting blood glucose levels. Metformin also helps to regulate the menstrual cycle.
In women who wish to become pregnant, Clomid (Clomid citrate) is usually the most commonly used drug to induce ovulation. Metformin is often used to increase the effectiveness of Clomid.
Physical exercise and weight loss are important as they work by improving insulin resistance, reducing the production of male hormones, and protecting against cardiovascular disease.
Differences between polycystic ovary and ovary cyst
Ovarian cyst and PCOS are completely different diseases.
In polycystic ovarian syndrome, the patient has multiple cysts of small size, about 5 mm (0.5 cm), scattered over both ovaries. Usually more than ten cysts are present in each ovary.
The ovarian cyst is different. It is usually a single lesion and of a larger size, usually more than 2 cm.