The two major thyroid (or thyroid) changes, hypothyroidism and hyperthyroidism, are diagnosed laboratorially by collecting blood to measure blood levels of basically two hormones, called free T4 and TSH.
Very succinctly, hypothyroidism is the disease caused by the insufficient production of thyroid hormones, whereas hyperthyroidism is the disease caused by the overproduction of thyroid hormones. Both diseases can be diagnosed through the measurement of thyroid hormones circulating in the blood. However, to understand what stands for acronyms like TSH, T3 and free T4, one must first understand how the thyroid works.
The thyroid is a butterfly-shaped gland located at the base of the neck. The thyroid picks up the iodine consumed in food and joins it to an amino acid called tyrosine to create two hormones, known as triiodothyronine (T3) and thyroxine (T4).
T3 and T4 synthesized by the thyroid are released into the bloodstream, where they act in all cells of our body, regulating their metabolism, that is, dictating how cells will turn oxygen, glucose and calories into energy. When the thyroid produces too much T3 and T4, our metabolism accelerates. When the thyroid produces little T3 and T4, our metabolism slows down.
In general, of the total hormones produced by the thyroid, 80% are T4 and 20% are T3. Despite being produced in less quantity, T3 is a hormone much more potent than T4, and its blood concentration is directly responsible for dictating the rhythm of the body's metabolism.
T4 is, in fact, a prohormone, that is, a precursor of T3. 80% of the T4 released into the bloodstream, on reaching organs or tissues such as liver, kidneys, spleen, muscles or fat is transformed into T3 for cell use. Therefore, T3 is effectively the thyroid hormone that acts in our body, having its origin predominantly in the circulating T4. Only a small portion of the active T3 is directly produced by the thyroid.
More than 99% of T4 and T3 circulating in the bloodstream are linked to a protein called TBG (thyroxine binding globulin). These hormones linked to TBG are innocuous and can not be used by organs and tissues. Therefore, only a tiny fraction called free T4 and free T3 are chemically active and can modulate the body's metabolism. Only free T4 is able to be transformed into T3 in organs and tissues.
To summarize:
1. Who effectively acts on the body cells modulating the metabolism is the hormone T3.
2. Much of the active T3 is derived from the conversion of T4 into the peripheral tissues.
3. Because more than 99% of T4 is bound to TBG, ultimately only a tiny fraction of less than 1% of free T4 is effectively the one that provides T3 for the organs and tissues of the body to use in their cells.
In conclusion, the blood free T4 dosage is the test that really gives us the notion of how much potentially useful thyroid hormone there is in the circulation. If there is too much circulating free T4, there will be a lot of T3 production in the organs, leading to hyperthyroidism. If there is little free T4 circulating, there will be a lack of T3 for the tissues, causing hypothyroidism.
In clinical practice, the free T4 dosage ends up being, in most cases, more useful than the free T3 or T3 dosage.
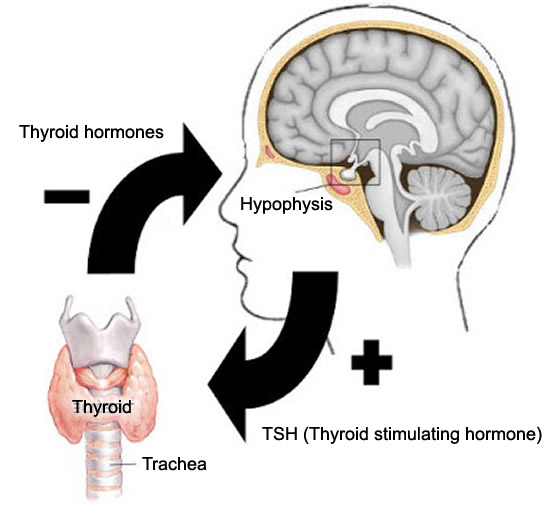
The amount of T3 and T4 produced by the thyroid gland is carefully controlled by the central nervous system, more specifically by the pituitary, a gland located at the base of the brain. In people with healthy thyroid, the amount of free thyroid hormones in the blood is always maintained so that there is neither excesses nor insufficiency. If there is too much T4 in the blood, the thyroid reduces its production of T3 and T4. On the other hand, if there are signs that free T4 levels begin to be insufficient, the thyroid quickly begins to produce more T3 and T4, so as not to let the body's metabolism slow down.
Thyroid function
The order for the thyroid to increase or reduce its production of T3 and T4 comes from the pituitary gland, through a hormone called TSH (thyroid stimulating hormone).
See figure beside and follow the reasoning. When there is little circulating thyroid hormone, the pituitary gland feels this deficiency and increases the secretion of TSH, giving order for a greater production of T3 and T4 by the thyroid. When T3 and T4 levels become satisfactory again, the pituitary gland feels this normalization and automatically reduces TSH production, thereby reducing the stimulation on the thyroid, preventing it from producing too much hormones.
The balance between TSH and free T4 levels is very delicate. The pituitary gland must always maintain an ideal TSH concentration, so that it prevents the thyroid from producing few hormones at the same time, nor does it stimulate it to produce too much hormones.
In the vast majority of cases, the dosages of TSH and free T4 are sufficient to allow us to evaluate how the thyroid function is functioning. Before we explain how to interpret the results of these two hormones, one must know what their reference values are (these values may change discreetly from one laboratory to another).
Normal TSH values: 0.4 to 4.5 mU/L
Normal values of free T4: 0.7-1.8 ng/dl
The current technique for detecting TSH is called ultra sensitive TSH, because unlike the first generations of this test, the ultra sensitive method can detect TSH levels as low as 0.1 mU/L.
TSH levels rise whenever the pituitary gland feels that there is a drop in thyroid hormone levels in the circulation. In patients with hypothyroidism, the pituitary gland needs to maintain TSH levels higher than normal (above 4.5 or 5 mU/L) in order to constantly stimulate the thyroid to increase its production of T3 and T4. From this point, we can have 3 different situations:
1. Subclinical hypothyroidism
If thyroid disease is still mild and elevation of TSH is able to stimulate the production of thyroid hormones in order to keep them at adequate levels, the patient will not present any symptoms, since the symptoms of hypothyroidism arise only when T4 levels are low. This is the case of subclinical hypothyroidism, which is an initial form of hypothyroidism.
Patients with subclinical hypothyroidism usually have slightly elevated TSH, between 5.0 and 10.0 mU/L, and a normal free T4, between 0.7-1.8 ng/dl.
2. Clinical hypothyroidism
If thyroid disease is more severe, however much the pituitary increases TSH production, the patient's thyroid will be unable to produce thyroid hormones in order to normalize blood levels. In these cases, the patient has elevated TSH, generally above 10 mU/L and low levels of free T4. Because your free T4 is low, the patient often has the typical symptoms of hypothyroidism.
Patients with untreated hypothyroidism may have very high TSH levels, sometimes above 100 mU/L.
3. Central hyperthyroidism
A completely different situation occurs when the patient has elevated levels of TSH, but also free T4. In this case, the problem is not in the thyroid, which responds adequately to the TSH stimulus. The problem is in the pituitary gland, which maintains elevated TSH production even though the patient already has elevated thyroid hormone levels in the circulation. As there is excess free T4, the patient has symptoms of hyperthyroidism. This form of hyperthyroidism, caused by pituitary dysfunction, is rarer than hyperthyroidism caused by thyroid disease.
The rationale for low TSH is the same for elevated TSH. If there is too much circulation of thyroid hormone in the blood, the pituitary gland reduces its release of TSH, decreasing the stimulus on the thyroid. In the same way, we can have 3 different situations:
1. Subclinical hyperthyroidism
If the thyroid is very active, the TSH levels fall so that the stimulus stops. In subclinical hyperthyroidism, TSH is very low, below 0.4 mU/L, but free T4 levels are normal. The patient therefore has no symptoms.
2. Clinical hyperthyroidism
Some diseases cause the thyroid to become excessively active and function independently of the pituitary gland, producing hormones even if there is no stimulus for TSH. The pituitary gland is stationary, with TSH levels of 0.1 mU/L (the lowest level we can measure), but free T4 is very high. These are the cases of clinical hyperthyroidism.
3. Central hypothyroidism
If TSH is very low, but T4 is free too, we are facing a healthy thyroid, which responds adequately to the lack of TSH. The problem will again be the pituitary gland, which, in the face of a low level of free T4, is unable to increase the TSH release in order to stimulate the thyroid to produce more hormones and prevent the patient from having hypothyroidism. This form of hypothyroidism, originating in the pituitary gland, is rarer than hypothyroidism caused by thyroid problems.
The diagnosis of hypothyroidism and hyperthyroidism, whether clinical or subclinical, is done in most cases only with TSH and free T4 levels. Eventually, free T3 levels may be required in more complex cases, which can not be explained here.