Tubal Ligation - Definition, Complications and Reversal
Tubal ligation, also called tubectomy, is a sterilization procedure that aims to prevent the woman from getting pregnant. Tubal ligation is considered a permanent contraceptive method and its success rate is very high, around 99%.
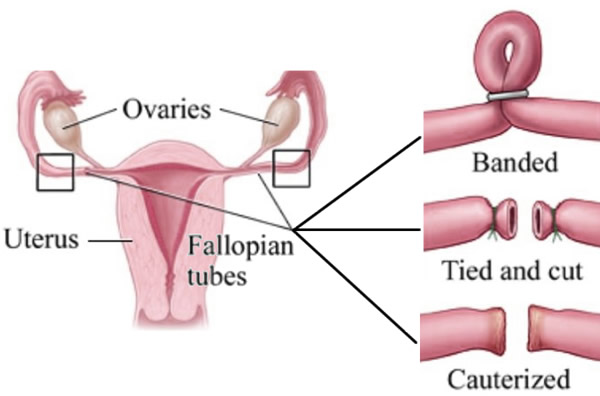
The female reproductive system consists basically of two ovaries, two fallopian tubes, a uterus and a vagina. The fallopian tubes, also known as uterine tubes, are a kind of tube that connects the ovaries to the uterus.
At each menstrual cycle one of the ovaries releases an egg to be fertilized. This egg is thrown towards one of the fallopian tubes, and there awaits the arrival of a spermatozoon for eventual fertilization.
Tubal tubal ligation works as a definitive contraceptive method because it is a procedure that causes interruption in the path of both tubes, thus preventing the sperm from reaching the ovum released by either of the two ovaries.
Binding of the fallopian tubes does not prevent ovulation or interfere with the female hormonal cycle, thus causing no change in the menstrual cycle.
There are currently three options for performing tubal ligation:
1. Laparoscopy
Laparoscopic laceration is a surgical procedure performed through a small incision near the navel and the lower abdomen, with the introduction of a device called the laparoscope, used to see the fallopian tubes. The doctor may use rings or clips to close the tubes. Another possibility is to cauterize them through heat.
2. Minilaparotomy
Minilaparotomy is a surgical procedure done immediately after delivery or up to two days later. The doctor makes a small incision in the abdomen and then removes a part of the fallopian tubes from each side. The procedure should not be done many days after delivery so that the uterus is still large, which facilitates surgery.
3. Hysteroscopic tubal ligation
Hysteroscopic tubal ligation is a non-surgical tubal ligation, which can be done outside the hospital setting with local anesthesia alone. This is currently the most suitable procedure for tubal ligation.
This type of ligation is done endoscopically through the vagina. There are two different methods:
Essure technology
In this procedure the endoscopic apparatus, called a hysteroscope, enters the vagina, traverses the uterus and reaches the tubes where it inserts a small spring called Essure.
The insertion of a foreign object into the fallopian tubes, such as the Essure, causes a reaction of the immune system, causing inflammation and subsequent growth of scar tissue, which causes the tubes to close.
This process of closing the tubes takes about three months to complete. After this period the woman performs an examination called hysterosalpingography, which consists of an x-ray of the female reproductive system after contracting. If Essure has caused effective tubal discontinuation, the contrast will not be able to reach the end of the tubes, proving complete obstruction of the uterine tube.
Surgical lachrymation, performed by laparoscopy or minilaparotomy, presents a complication rate of 0.1%. The most common include infection, bladder or bowel injury, internal bleeding or problems related to anesthesia.
The complication rate with hysteroscopic sterilization is about 0.002%. The most common complication is a lesion of the uterine wall, a problem that usually does not cause major problems, even because the patient who undergoes the tubal ligation does not intend to become pregnant anymore.
The three techniques of tubal ligation have a success rate above 99%. There are studies that show that after 15 years of tubal ligation, less than 1% of women eventually became pregnant. The big problem is in most cases the pregnancy ends up being ectopic (tubal pregnancy). Therefore, every lacquered woman should immediately seek her gynecologist if she has a delayed menstrual period.
Tubal ligation does not alter the menstrual cycle or interfere with a woman's sexual desire.
Repentance over definitive sterilization usually occurs in women who have had tubal ligation as young as 25 years. They are women who often separate, marry again, and begin to want to have a child with their new husband.
Ligation is considered a definitive sterilization. In some cases reversal is possible, but there are risks and the procedure is much more complex than tubal ligation. The success rate of the reversal is only 20%. Therefore, if the patient has any doubts or insecurity, the tubal ligation should not be the contraceptive method of choice.