Meniere's Disease - Causes, Symptoms and Treatment
Meniere's disease, also called endolymphatic hydrops is a disorder of the inner ear which causes episodes of vertigo, progressive hearing loss and ringing in the ears.
Individuals between the ages of 40 to 50 years are the most affected, but the Meniere's disease can occur at any age, even in children.
Although Meniere's disease is considered a chronic disease, since there are several forms of treatment that can help relieve symptoms and minimize the impact of long-term illness.
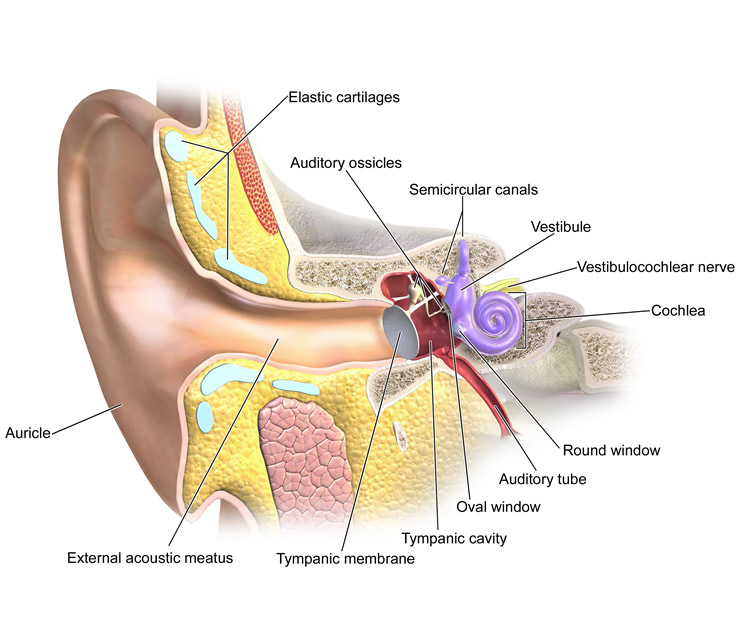
To understand the Meniere's disease is necessary to have at least a basic understanding of the anatomy and physiology of the inner ear, where is the maze, which is responsible for maintaining balance.
The maze is a set of semicircular arcs having liquid inside called endolymph. The movement of these liquids, which occurs whenever we move or change position, is transformed into electrical signals that go to the brain where they are interpreted in order to identify our real position in space.
Through these signals, the brain can know whether we are still in motion acceleration or deceleration, up or down, straight or making curve, side, standing, lying, etc. Thanks to the correct interpretation of the data obtained through the movement of endolymph is that we always keep us in balance, even with eyes closed.
Meniere's disease arises when, for reasons not yet elucidated, an increase of the volume of the endolymph inside the maze, causing distention of this compartment by increasing the internal pressure.
Infections, head trauma, migraine, immune system disorders, anatomical variations of the inner ear or genetic predisposition are some of the changes that can lead to increased endolymphatic pressure.
Regardless of the cause, this change of internal ear pressure causes the signals sent to the brain become more inaccurate, which explains the occurrence of symptoms such as dizziness and imbalance.
The terms of Meniere disease and Meniere's syndrome are often used interchangeably. In fact, there is little difference. The term Meniere's syndrome is more properly applied when the cause of the increased pressure inside the maze is known, for example, in cases that arise after head trauma. Already the term Meniere�s disease should be used preferably when the increase in endolymphatic pressure comes with no identifiable cause.
One in ten patients who complain of vertigo symptoms have disease or Meniere�s syndrome.
Vertigo is a type of dizziness specific that causes the sensation of the surrounding environment be spinning. Dizziness roundabout is similar to what we feel when we turn on our own axis several times and then stopped suddenly.
If you want to read about other common causes of dizziness or lightheadedness, visit the links above.
The symptoms of Meniere's disease are intermittent, or come and go over time. Sometimes the remission period lasts several months. In general, only one ear is affected, but bilateral involvement is not impossible.
During crises, episodes of vertigo can last from 20 minutes to 24 hours. Nausea and vomiting are very common in the acute phase of dizziness. At the time of crisis, the patient is incapacitated, because besides the severe nausea, it also has great difficulty in maintaining balanced. This feeling of imbalance may still remain for a few days, to a lesser degree, after the resolution of vertigo.
Hearing loss is fluctuating, with alternating periods of deterioration and spontaneous improvement. Low frequency sounds are initially the most affected. Over time, however, every crisis, the patient loses permanently some of his hearing. Over 10 years of disease that may result in significant hearing loss at all frequencies of sound.
Although we call tinnitus, which the patient with Meniere's disease hears, in most cases, it is not a sharp sound, but a similar feeling with the sea of noise we hear when we place a large shell in the ear. Therefore, tinnitus or tinnitus terms are best suited to describe the "buzz" that Meniere's disease causes. Tinnitus can be continuous or intermittent. Over time, patients who experience tinnitus can notice that loud sounds become distorted.
The severity of Meniere's disease varies from case to case. In some dizziness are violent, keeping the patient all day bed and several episodes of vomiting. In others, the picture can be mild, causing nuisance, but not disability.
Attacks can be triggered by stress, menstrual cycle, cigarette or changes in diet. Before arise vertigo crises, it is common for the individual feel a clogged ear. Over the years, the patient can learn to recognize a crisis approaching.
The fact of vertigo is intense not necessarily mean that the tinnitus and hearing loss also will be. Especially in the early years of the disease, the presentation of the picture varies greatly from one individual to another.
In many cases, Meniere's disease cure by itself. After 8 years, over 70% of patients are permanently free of symptoms. The problem is that after so many years, a lot end up developing partial loss, but permanent, hearing and balance.
There is no examination or specific test to diagnose Meniere's disease. In general, the diagnosis is made by physical examination and medical history of the patient. Sometimes, the patient remains with varying degrees of hearing symptoms and dizziness for up to three years before you can find a doctor to establish the correct diagnosis.
The diagnostic criteria proposed by the American Academy of Otolaryngology and Head and Neck Surgery is currently the most used to define the diagnosis of Meniere's disease. Are they:
History of at least 2 episodes of vertigo lasting at least 20 minutes.
Hearing loss confirmation by audiometric testing.
Presence of tinnitus.
In addition to these criteria, it is also important to rule out diseases that may cause similar clinical features, such as multiple sclerosis, acoustic neuroma, diabetes mellitus, thyroid disease and other diseases of the inner ear.
There is no cure for Meniere's disease, but no effective treatment for the symptoms in most cases.
In general, the goals of treatment of Meniere's syndrome are:
Reduce the frequency and severity of attacks of vertigo.
Relieving chronic symptoms such as tinnitus and balance problems.
Try to prevent the progression of the disease, especially hearing loss and imbalance.
Vertigo attacks can be controlled in up to 95% of patients, although the progressive hearing loss rarely respond to treatment. Cases with better results are often those who were referred early to an ENT specialist.
In addition to medical treatment itself, some lifestyle changes are also important. In many cases, Meniere's syndrome seizures may be triggered by factors such as consumption of caffeine, alcohol, excess salt ode, nicotine, stress, allergic reactions. Avoiding these triggers is essential to control the disease.
Medications for Meniere's syndrome
During the crisis, the treatment aims to improve the vertigo and relieve nausea. Drugs such as diazepam, lorazepam, meclizine, dimenhydrinate, scopolamine, prochlorperazine, promethazine, and the most often utilized for these purposes.
After the crisis, some medications should be used to control long-term disease. Diuretics such as hydrochlorothiazide, and betahistine are vasodilator drugs with better long-term results.
Other treatment for long term control of disease include:
Vestibular rehabilitation therapy, which are specific exercises in order to help your body to maximize balance.
Use of hearing aid for patients with permanent reduction of hearing.
Therapy Meniett device, which is a device used for application of positive pressure in the middle ear in order to improve the exchange of fluid in the labyrinth. This treatment is carried out at home, usually three times per day with sessions lasting 5 minutes.
Destructive surgery and procedures
For patients with unilateral Meniere's disease and who have not shown significant improvement with the previously described treatments, the use of a procedure that causes irreversible damage to the patient maze is an option. The goal is to make, being one of the destroyed labyrinths, the brain pass only use the information provided by the other ear, which is healthy, to keep the balanced individual.
The destructive procedure may be done by gentamicin dexamethasone injection or directly into the middle ear. Gentamicin is more effective, but the risk of it that aggravate hearing loss ear.
In severe and untreatable cases, surgery to remove the diseased labyrinth called labyrinthectomy is the option. This procedure however, should be done only in extreme cases because it causes deafness in the affected ear.
A less extreme option is the surgical section of the vestibular nerve. This procedure aims to cut the nerve that carries the maze information to the brain. In this case, the hearing of the affected ear is preserved. The problem is that this surgery is much more complex and higher rate of complications than labyrinthectomy.
One way of nondestructive surgery is called decompression of the endolymphatic sac. In this procedure, the surgeon removes a part of the mastoid bone, increasing thereby the space for expansion of the endolymph within the inner ear. This procedure although less effective than the destructive techniques presents much lower rate of complications. It usually is reserved for patients with intractable vertigo, but still intact hearing.