Streptococcal Pharyngitis - Symptoms, Diagnosis and Treatment
Neck pain is a very bothersome symptom, which usually occur in both adults and children. Overall, the sore throat is caused by an inflammation of the tonsils or pharynx, frames called tonsillitis and pharyngitis, respectively. When both are inflamed, very common situation, we say that the patient has a tonsillitis.
In most cases, neck pain originates from an infection. Pharyngitis, and viral tonsillitis are the most common causes of sore throat, but bacterial infections are also common sources of inflammation in the throat.
Among the bacteria that cause pharyngitis or tonsillitis, the Streptococcus pyogenes (Streptococcus group A) is what deserves more emphasis, not only for being the most common form of bacterial tonsillitis, but also because it is the form of throat infection that causes more complications. The Streptococcus pyogenes is responsible for about 30% of cases of pharyngitis 10% in children and in adults.
In this article we will talk specifically of tonsillitis and pharyngitis caused by Streptococcus pyogenes . We will address the symptoms and forms transmissions, diagnostic methods, potential complications and treatment options.
What is streptococcus pyogenes - streptococcus group A
The bacteria of the genus Streptococcus has several different species, many of them capable of causing infections in humans. One way of example, Streptococcus pneumoniae is a common cause of pneumonia, Streptococcus agalactiae can cause serious infections in newborns and Streptococcus viridans is a common cause endocarditis.
The Streptococcus pyogenes, target of our article, is also known as Streptococcus group A beta-hemolytic A. This species of Streptococcus is the most common cause of sore throat caused by bacteria. That is, if a patient has a sore throat caused by bacteria, the chance of this bacterium be Streptococcus pyogenes is very large.
But Streptococcus pyogenes not only causes pharyngitis and tonsillitis, it can also be responsible for other infections such as impetigo, erysipelas and psoriasis guttata, a rare form psoriasis. In this article, however, let us focus only on pharyngitis and its complications.
The bacterium Streptococcus pyogenes is highly contagious and can be transmitted through coughing, sneezing, saliva droplets emitted during speech or the cutlery or sharing cups. Hands contaminated by respiratory secretions are also an important vehicle for the transmission of group A streptococcus.
Generally, children between 3 and 14 years are the group most at risk of contamination. However, not all people who become infected with Streptococcus pyogenes will develop inflammation of the throat. Adults often come into contact with the bacteria and not develop symptoms.
There are also cases of patients who come in contact with Streptococcus pyogenes , they do not develop symptoms, but become carriers in the bacteria in the oropharynx. In the winter season, during which people get more time together indoors, about 20% of school children become asymptomatic carriers of Group A Streptococcus in their orofaringes.
These asymptomatic carriers may remain with the bacteria for several months without any problems. In many of these carriers, the bacterium becomes active only when the patient develops a viral respiratory infection. In these cases it is very difficult to distinguish between a pure viral pharyngitis or an opportunistic bacterial pharyngitis, who took advantage of an inflammation caused by a virus to become active.
These carriers tend not to be a source of transmission of the bacteria while they are asymptomatic. However, if at any time the bacteria becomes active and causes the throat infection, the risk of contagion becomes real.
The incubation period Streptococcus pyogenes, ie the time between infection and the appearance of the first symptoms is 24 to 72 hours but may be as long as 2 weeks in some cases.
The main symptoms of pharyngitis and / or streptococcal tonsillitis are sore throat, fever, headache and redness of the throat and tonsils. This signs and symptoms, however, do not help much in diagnosis because they are common to almost all types of pharyngitis, especially those of viral pharyngitis.
In fact, it is not always easy to distinguish a streptococcal pharyngitis pharyngitis of viral origin. However, some findings on physical examination can help. For example, the following signs speak much in favor of pharyngitis Streptococcus pyogenes:
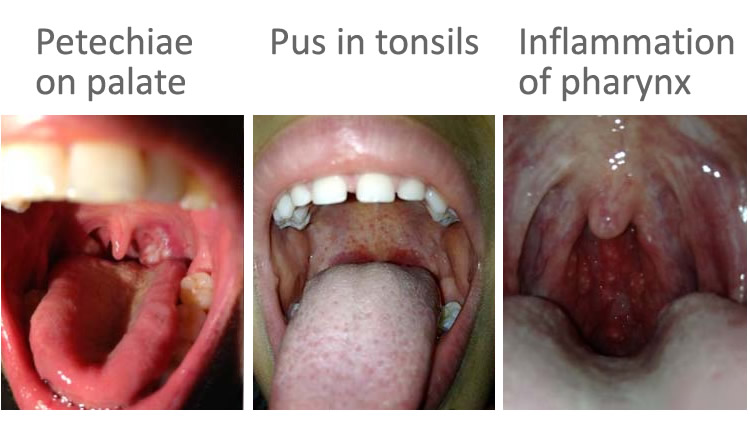
Tonsils swollen and pus (presence of plaques or white spots on the tonsils or pharynx)
Pharynx inflamed and pus points.
Enlarged and painful lymph nodes in the front of the neck just below the jaw.
Presence of petechiae on the palate (several red dots on the roof of the mouth).
Inflammation and swelling of the uvula (buzzer or bell neck).
Abrupt onset and rapid development of symptoms.
On the other hand, the presence of typical symptoms of viral infection, such as sneezing, cough, runny nose, hoarseness, conjunctivitis, diarrhea, or mouth ulcers, more direct diagnostic viral pharyngitis, such as a cold or flu.
However, as previously mentioned, a patient is quite possible to develop a bacterial pharyngitis the middle of a respiratory viral infection, which makes the distinction between inflammations of vital source throat and bacterial very difficult.
More specific signs of pharyngitis / tonsillitis bacterial are petechiae on the palate and the presence of pus in the tonsils or pharynx. Still, none of them allows us to say with 100% certainty that we are facing a bacterial pharyngitis, for 5 to 10% of non-bacterial throat inflammations can have these signs.
Therefore, at least 50% of cases of inflammation of the throat for a specific set of symptoms and signs enough to allow the physician make the diagnosis of streptococcal pharyngitis only with the physical examination. In most cases, the diagnostic certainty is obtained only through additional tests such as the rapid test or pharyngeal material culture, which indicate the presence of Streptococcus pyogenes in the oropharynx, as we shall see later.
The streptococcal pharyngitis frame usually has a finite duration. Usually neck pain disappears within five days, even without treatment with antibiotics. Still, treatment with antibiotics is indicated, especially in children, because it reduces the duration of disease, relieve symptoms and, most importantly, reduces the risk of complications.
The big problem of streptococcal pharyngitis is usually not the sore throat itself, but the risk of complications. Children are the main victims of these complications, they are the group that most needs treatment with antibiotics for prevention.
Some complications are severe, even life-threatening, as in the case of streptococcal toxic shock syndrome. Others may cause injury to internal organs such as the kidneys in the case of post-streptococcal glomerulonephritis, or heart in rheumatic fever. There are also simpler situations, such as scarlet fever, which is a skin rash that is usually benign and easy treatment.
Among the possible complications of streptococcal pharyngitis, we can highlight:
It is important to note that most cases of streptococcal pharyngitis course without complications. However, as some of these problems are serious, antibiotic use turns out to be indicated for prevention, especially in children.
Identify correctly if pharyngitis is bacterial, viral or non-infectious origin is important when devise strategies aimed at preventing complications and interruption of contagion to others, while minimizing the unnecessary use of antibiotics in children and adolescents who have inflammation throat of non-bacterial origin, which represents the majority of cases.
Currently, the most used way to detect a streptococcal pharyngitis is through the rapid detection test group streptococcus A. This test is done using a swab (swab), which is a kind of long cotton swab that is used to gather material tonsil (see picture). This test can identify the presence of Streptococcus pyogenes in the oropharynx and the result is obtained in a few minutes. If the test is positive, the patient should be treated with appropriate antibiotics.
If the test is negative but the suspicion of streptococcal pharyngitis is very strong, the material collected by swab can be sent for culture, which is a more reliable method than the rapid test. The downside of culture is the fact that the result only be available after 48 hours.
The goal of treatment with antibiotics aimed at eradication of group A streptococci of the oropharynx. The elimination of bacteria brings the following benefits:
Reduction of the duration and severity of signs and symptoms.
Reduction in the incidence of complications.
Reduction of bacteria transmission risk to others.
With only 12 to 24 hours after initiation of antibiotic treatment, the majority of patients are no longer able to transmit the bacteria to other people. This means that the child can return to attend school the next day to the beginning of treatment, if feel good. Regarding symptoms, improvement is felt within 24 to 48 hours after onset of antibiotic.
Derivatives of penicillin antibiotics should always be the first choice of treatment because they are the most effective. The most suitable schemes are:
Penicillin benzathine intramuscularly in a single dose in the dose of 600,000 U for patients with less than 27 kilograms or 1,200,000 U for those with more than 27 kilos.
Penicillin V orally at a dose 250 mg 2 or 3 times per day for children or 500 mg 2 times a day for adults. Treatment should last for 10 days.
Amoxicillin orally at a dose of 25 mg / kg (maximum dose of 500 mg per serving) 2 times per day. Treatment should last for 10 days.
Among the three options above, the best of all is benzathine penicillin as it is the simplest administration and is the most effective in preventing complications, especially rheumatic fever in children.
Amoxicillin can be taken with or without clavulanic acid, depending on the streptococcal resistance profile in the community that the patient lives.
Cephalexin orally at a dose of 20 mg / kg (maximum dose of 500 mg per serving) 2 times per day. Treatment should last for 10 days.
Azithromycin orally at a dose of 12 mg / kg (maximum dose of 500 mg per serving) 1 time per day. Treatment should last for 5 days.
Clarithromycin orally at a dose of 7.5 mg / kg (maximum dose of 250 mg per serving) 2 times per day. Treatment should last for 10 days.
Most people improvement within 48 hours, but it is essential that the treatment is continued until the end, even if the patient is already completely asymptomatic. The interrupt before the end of the antibiotic increases the risk of the occurrence of complications. As benzathine penicillin is the only treatment done with a single dose, it is the option most successful and adherence rate.
In addition to the antibiotic, the patient may also be treated with anti-inflammatory or analgesic, for the control of symptoms while antibiotics have no effect.