Systemic lupus erythematosus (SLE) is an autoimmune disease of unknown cause that can affect the skin, joints, kidneys, lungs, nervous system and other body organs.
An autoimmune disease is one when the immune system mistakenly begins to produce antibodies against structures of our own body. They are called autoantibodies.
It is important to know that patients with lupus not necessarily present all symptoms described below. The clinical course of SLE is highly variable and can be characterized by periods of remissions and relapses. The disease can worsen or improve over years, and symptoms that never existed can arise from one moment to another.
The severity of lupus depends on which organs are affected and how. There is also a scale of severity regarding the involvement of a single organ, for example, lupus lesions can cause very severe renal pain or be virtually asymptomatic. Patients with severe injuries to various organs usually have a poor prognosis. But patients with mild and limited to one or few organs can have practically normal life for decades.
Constitutional symptoms are symptoms of nonspecific signs and symptoms that affect various systems of the body and are common to many diseases. The main feature of constitutional symptoms is to give us the idea that there is something wrong with the health, but without indicating precisely the source of the problem.
Systemic lupus erythematosus is a disease that usually manifests with constitutional symptoms in its early stages. Among them the most common are:
Fatigue and exercise intolerance - these symptoms are extremely common and affect more than 80% of lupus patients
Muscle pain and feeling weak
Weight loss - occurs unintentionally and is usually associated with loss of appetite
Fever
It is worth talking a bit more about fever. Fever in systemic lupus can occur when the disease is active or because there is an ongoing infection. Fever in lupus, or caused by disease and not by infection, is usually low and associated with other symptoms of lupus which will be explained later in the text.
Patients with lupus have a higher susceptibility to infectious diseases, fever may be a sign of infection in progress. The fever caused by infection is usually higher and associated with other typical symptoms, such as cough and expectoration in pneumonia, meningitis, neck stiffness, lower back pain in kidney infections (pyelonephritis), etc.
If the patient already has systemic lupus, it is likely that he/she is being treated with anti-inflammatories or steroids, drugs that decrease inflammation and inhibit lupus fever. In this group of patients the presence of fever should raise the suspicion of an ongoing infection.
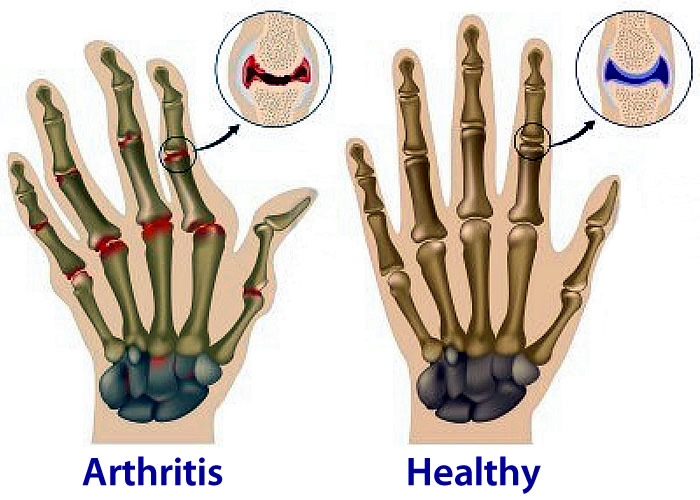
Approximately 95% of lupus patients will present involvement of joints at some point in their life. The articular manifestations are the most common arthralgia (joint pain without inflammation) and arthritis (joint inflammation) and usually present in the early stages of lupus.
Arthritis in lupus has some characteristics:
It is a polyarthritis - affects more than four joints simultaneously
It's a symmetrical arthritis - usually affects both knees, elbows, ankles and other joints simultaneously
It is migratory - inflammation of a joint can disappear in just 24 hours and emerge in another one
It does not usually cause serious deformities or arouse prolonged morning stiffness, as in rheumatoid arthritis
The pain is disproportionate to the physical appearance of the joints
Up to 75% of patients with lupus will develop some kidney injury during the course of their disease. The most common finding is the loss of protein in urine, called proteinuria, characterized by an excessive foaming urine.
Renal involvement in lupus
Other signs and symptoms of renal involvement in lupus are:
Hematuria (blood in the urine), which may or may not be visible to the naked eye
Elevation of blood creatinine, a sign of kidney failure
The renal involvement is the most common glomerulonephritis (kidney glomerulus injury) caused by autoantibodies. There are basically five types of glomerulonephritis in lupus, lupus nephritis gathered by term. They are:
Lupus nephritis class I - minimal mesangial glomerulonephritis
Lupus nephritis class II - proliferative mesangial glomerulonephritis
Lupus nephritis class III - focal proliferative glomerulonephritis
Lupus nephritis class IV - diffuse proliferative glomerulonephritis
Lupus nephritis class V - membranous glomerulonephritis
Classes III, IV and V are the most serious, with the diffuse proliferative glomerulonephritis (class IV) having the worst prognosis. The minimal mesangial glomerulonephritis (class I) is the mildest.
Lupus nephritis is classified into classes because each of these lesions presents different treatments and prognosis. Therefore, identifying which type of lupus nephritis the patient has is very important.
It is not possible to identify which type of lupus nephritis is dealt with only with clinical data, as proteinuria, hematuria and renal nephritis are common findings in type II, III, IV and V. Therefore, all patients with lupus manifesting signs of kidney disease should be subjected to renal biopsy to identify which type of injury in the glomerulus causes autoantibodies. It is possible that a patient has more than one class of lupus nephritis simultaneously.
Classes I and II do not usually require specific treatment, however, the classes III, IV and V have a worse prognosis and a high risk of terminal renal failure is usually treated with immunosuppressive drugs. The most common are corticosteroids (cortisone), cyclophosphamide, cyclosporine, mycophenolate mofetil and azathioprine.
Untreated patients or those having no good response to drugs inevitably end up needing hemodialysis.
Skin is another very commonly affected organ. Up to 80% of lupus patients have some type of skin involvement, especially in sun-exposed areas. Typical lesions include malar rash or butterfly rash. It is a reddish area that covers the cheeks and nose.
The malar rash appears on at least 50% of patients, usually lasts a few days and there is always recourse exposure. Prolonged exposure to fluorescent lights can also trigger skin lesions.
Another common skin lesion is discoid lupus, which is characterized by rounded and reddish plaques, most commonly on the face, neck and scalp. The discoid lupus may be part of the framework of systemic lupus, or be the only manifestation of the disease. In the latter case, the prognosis is better, as there is no involvement of other organs.
Patients with discoid lupus have 10% chance of progression to systemic lupus erythematosus. The more numerous lesions are discoid, the greater is the risk of progression to other organs.
Other common skin lesions are hair loss, which can affect not only the scalp, but also eyebrows, eyelashes and beard. Oral ulcers similar to canker sores are common, however, with the difference being usually painless.
Autoantibodies can also attack the blood cells produced by the bone marrow. The most common is anemia, which occurs not only by the destruction of red blood cells, but also by inhibiting the production in the bone marrow.
Another common hematologic change is a decrease in white blood cells (leukocytes), called leukopenia. The mechanism is the same as anemia, destruction and inhibition of its production. Following the same reasoning we can find the reduction in the number of platelets, called thrombocytopenia.
When there is a drop in the three bloodlines (erythrocytes, leukocytes and platelets) it is called pancytopenia. These changes can be detected by examining blood count.
Any of these alterations in blood cells can be lethal, either by severe anemia, infections due to low WBC counts or spontaneous bleeding due to falling platelets. Lymph node and spleen are also a common finding in lupus and can be confused with lymphoma.
Blood vessels, particularly the arteries, are also often affected by lupus.
Raynaud's phenomenon is a change in color of the limbs, usually hands or feet, caused by spasms of blood vessels. The spasm of the arteries causes a sudden lack of blood leaving the pale hand. If the spasm persists, the lack of blood causes the hand that was pale start getting purple. This ischemia can cause a lot of pain. When the spasm disappears, the rapid return of blood leaves the skin hot and red.
Raynaud's phenomenon is not exclusive to lupus and can occur even in people without any diagnosed illness. Cold, cigarettes and caffeine can be triggers for this symptom.
Another common vascular problem in lupus is the occurrence of thrombosis. The antiphospholipid syndrome is a disease that occurs frequently in patients with lupus and is associated with the formation of multiple thrombi in both the arteries and veins, which can lead to conditions such as stroke, renal infarction, limb ischemia, venous thrombosis of the legs and pulmonary embolism.
Apart from thrombosis occurring with the antiphospholipid antibody syndrome, the autoantibodies of lupus can attack the blood vessels directly, causing vasculitis. Vasculitis can affect any vessel in the body and can injure skin, eyes, brain, kidneys etc.
Eyes are organs commonly affected by lupus. The most common manifestation is keratoconjunctivitis sicca, also known as dry eye syndrome, very common in Sjögren's disease, but it can also be a symptom of lupus.
Other symptoms of lupus-related vision are retinal vasculitis, uveitis (inflammation of the iris, the colored part of the eye) and episcleritis (inflammation of the sclera, the white part of the eyes).
Lupus can present with neurological and psychiatric syndromes. Among neurological injuries thrombosis and vasculitis are common, which eventually cause stroke.
Psychiatric disorders can also occur due to lupus. The most common psychosis is when the patient starts having bizarre thoughts and hallucinations, and dementia, with progressive loss of memory and ability to perform simple tasks.
The lung and pleura are also organs susceptible to lupus. Pleural effusion, pneumonitis, interstitial lung disease, pulmonary hypertension and alveolar hemorrhage are the most common pulmonary manifestations. As has been explained above, pulmonary embolism is a complication that can develop in patients with antiphospholipid antibodies.
Heart disease is common among patients with systemic lupus erythematosus. Cardiac involvement may manifest as:
Valvular disease, most often as a mild mitral regurgitation
Endocarditis (inflammation of the heart valves) noninfectious, called Libman-Sacks
Disease of the pericardium (the thin membrane that surrounds the heart). The most common manifestation is pericarditis, inflammation of the pericardium