Fulminant infarction is one of the leading causes of sudden death. After a heart attack, the heart can stop working because it has suffered necrosis in an extensive area of your muscle or because a malignant arrhythmia has arisen. In both cases, the heart becomes unable to pump the blood properly, leading the patient to circulatory collapse, which is a situation in which the organs and tissues of the body do not receive blood properly.
In this text we will explain how a heart attack arises, which is a malignant cardiac arrhythmia and why some people have a heart attack and can reach the hospital on time, while others have a sudden death infarct.
We call a fulminant infarct that causes the death of the patient before there is time for a medical care, that is, the patient dies before arriving at the hospital. About 15% of infarcts manifest themselves with sudden death, giving no chance to the patient. Fortunately, the other 85% can make it to the hospital on time.
Let's start with the basics. Any cell in our body needs blood to live; when an artery suffers a sudden obstruction of the blood flow, the tissues nourished by the same suffer ischemia and necrosis. To this death of a tissue we give the name of infarction. An infarction can occur in the brain, kidney, lung or any other organ of the body. Heart attack, or myocardial infarction, therefore, means death of the heart muscle cells (called myocardium), due to lack of blood supply.
The arteries that carry blood to the tissues of the heart are called coronary arteries. Our heart has two major arteries responsible for the cardiac blood supply: the left coronary artery, which nourishes the left side of the heart, and the right coronary artery, which nourishes the right side of the heart. For all cardiac tissue to receive blood, these coronary arteries need to branch out, forming a large web of blood vessels around the entire heart.
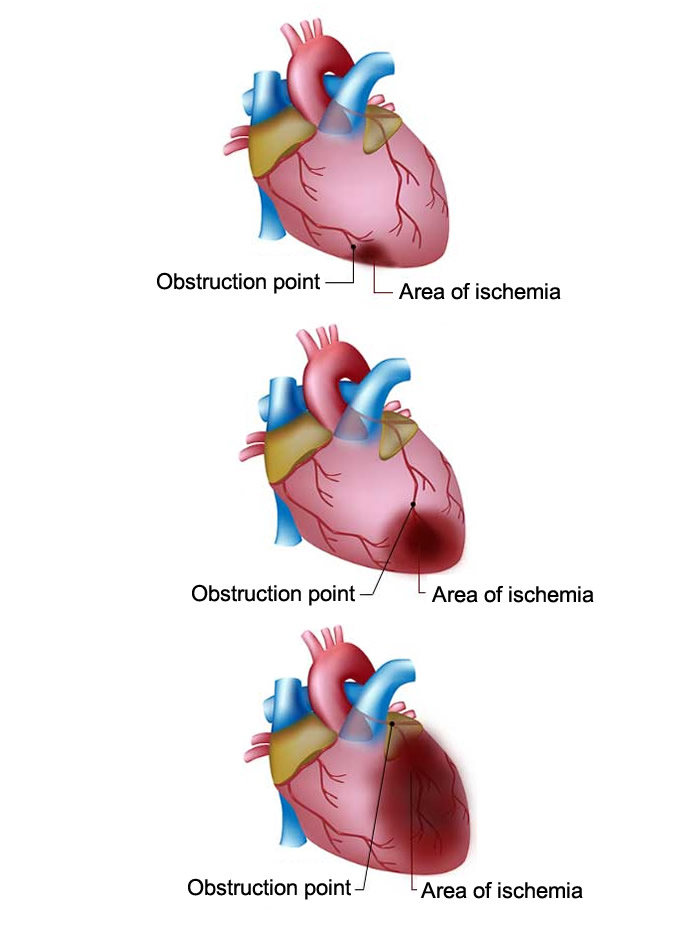
The larger the infarcted area, ie, the more extensive the muscle region that suffered necrosis due to lack of blood nourishment, the greater the severity of the infarction. Look at the illustration below for an example of 3 different locations for an obstruction of the coronary arteries and their consequences.
It is possible to notice that the closer to the birth of the coronary arteries the obstruction occurs, the greater the affected area. It is not difficult to understand why the obstruction in the third figure is much more serious than in the first. All that necrotic muscle becomes useless and unable to contract to pump the blood. When we suddenly lose our blood pump, we collapse, which is called circulatory shock.
In addition to the circulatory shock, called in this specific case of cardiogenic shock because it originates in the heart, there is another important cause for a rapid death after a heart attack: cardiac arrhythmias. The cardiac tissue that suffers from infarction can no longer transmit the normal electrical impulses of the heart, causing disturbances in electrical conduction, which favors the appearance of serious cardiac arrhythmias. Malignant arrhythmias are the main cause of sudden cardiac death. More than 70% of these occur due to ischemic heart disease.
In fact, an extensive heart attack is a major risk, but it is not the only cause for cardiac arrest. Several small infarcts accumulated over the years or a single ischemia, even if not very extensive, but located capriciously in a prime area of the generation and transmission of electrical impulses of the heart can also trigger malignant arrhythmias, leading to cardiac arrest. Therefore, two factors are important in the prognosis of an infarct: size and location of the affected area.
We call that malignant arrhythmia that does not produce the electrical impulses necessary for the correct heart beat. The heart works in a very synchronized way. If the electrical impulses do not arise at the right time and are not transmitted properly, the heart will not be able to contract and pump the blood properly.
The main arrhythmia responsible for cardiac death is ventricular fibrillation . During ventricular fibrillation, the electrical stimuli become chaotic, being unable to generate a contraction of the cardiac muscle in a synchronized way; the heart simply begins to shake and can no longer pump blood to the rest of the body. A heart in ventricular fibrillation is basically a still heart, subject to a storm of useless electrical impulses.
After a few minutes in ventricular fibrillation, the tissues of the rest of the body begin to die, including the brain. A person with ventricular fibrillation is technically dead and needs to be resuscitated immediately, before the brain dies from lack of blood circulation. If not promptly reversed with a defibrillator (electric shock), the patient will die in a matter of minutes.
When the patient is in ventricular fibrillation, only heart massage is not enough to save their life. That is why in recent years, airports, airplanes, concert halls, shopping malls and other places with a large public movement have made electric defibrillators available for the eventual case of sudden cardiac arrest in their establishments.
The patient usually begins a picture of tiredness, sweating and chest pain, just like any other heart attack. If the affected heart area is too large, the heart collapses, and the patient rapidly evolves into cardiogenic shock, which is characterized by hypotension and intense shortness of breath. If the patient has a malignant arrhythmia, he loses consciousness and stops breathing. The picture is dramatic because, as already said, ventricular fibrillation is a form of cardiac arrest.
It is important to note that the arrhythmia may appear at any time. In some patients it appears soon after the onset of symptoms; in others, it may appear only after a few hours after the onset of the infarction, often with the patient already inside the hospital, which, in this case, greatly increases the chances of reversion of the condition.
Any patient with sudden chest pain should be evaluated by a physician. It is impossible, without medical evaluation, to predict which infarction will progress well or badly, based only on the first symptoms.
Is it possible to predict a fulminant heart attack before the infarction arises?
It is not always possible to predict with great advance who is at risk of fulminant infarction. The main risk factors are the same for any heart attack:
The more risk factors a person has, the more likely he or she will have coronary disease, increasing the risk of a more extensive heart attack. Patients with many risk factors, especially if they are men over 50 years of age, should be evaluated by a cardiologist.
When coronary obstruction is slow and pre-progressive, the patient begins to experience symptoms of decreased blood supply to the heart. It is called angina, a pain in the chest that arises from exertion or in periods of stress, and disappears at rest. Angina is a transient ischemia caused by a partial obstruction of the coronary arteries. Blood gets to the heart muscle in lesser amounts, but is not reduced enough to cause a necrosis.
Patients with angina usually seek medical attention before there is complete obstruction of the coronary arteries, and through cardiac catheterization they can identify and correct obstructions in time before they have a stroke.
Through catheterization, also called coronary angiography, it is possible to map all vessels of the heart. If the doctor finds, for example, an artery with 80% or 90% of obstruction, we already know in advance that this patient is on the verge of a heart attack. This obstruction needs to be run through an angioplasty. Some patients have such serious coronary lesions that they need surgery, called the saphenous vein, to replace the diseased arteries.
Patients who have previously had previous infarcts, having several small areas of necrotic cardiac tissue or heart failure, are at great risk for malignant arrhythmias. Through studies of the heart's electrical activity, the physician can recognize who the patients are at high risk for malignant arrhythmia.
In these cases, the cardiologist may indicate the placement of an implantable defibrillator, which is a small device, similar to a pacemaker, capable of recognizing the onset of a cardiac arrhythmia. When the patient enters a malignant arrhythmia, the defibrillator recognizes the problem and saves its life, releasing immediately an electric shock capable of abort the arrhythmia.
However, not all patients have some type of symptom before the infarction. Therefore, I repeat, the evaluation of a cardiologist is always necessary in people with risk factors.
If the patient suffers from cardiac ischemia and evolves with a malignant arrhythmia out of a hospital environment, the chances of surviving are very small. Ventricular fibrillation needs to be reversed with a defibrillator within minutes. After 10 minutes of fibrillation, most patients will no longer be able to be saved, even if electric shock from the defibrillator is given. In addition, the longer the patient remains in cardiac arrest without medical care, the greater the risk of irreversible damage to the brain. As long as the heart is stopped, the brain will not receive blood.
It is due to this urgency in the treatment of malignant arrhythmias that, as already mentioned, some public places already have automatic defibrillators. In general these machines are of simple handling and can be operated by lay people; simply connect the paddles to the patient's chest as indicated, switch on the machine and move away. The rest of the work she will do alone.
If the patient has previously been evaluated by a cardiologist and has an implantable defibrillator, it will probably save his life, as the shock will come immediately after the arrhythmia begins.
It is important to note that arrhythmia reversal is only the first step in the treatment of severe infarction. This patient does not stop having a heart attack just because the arrhythmia has been treated; he needs to be hospitalized and may still die from various other complications of the infarction, such as severe heart failure.